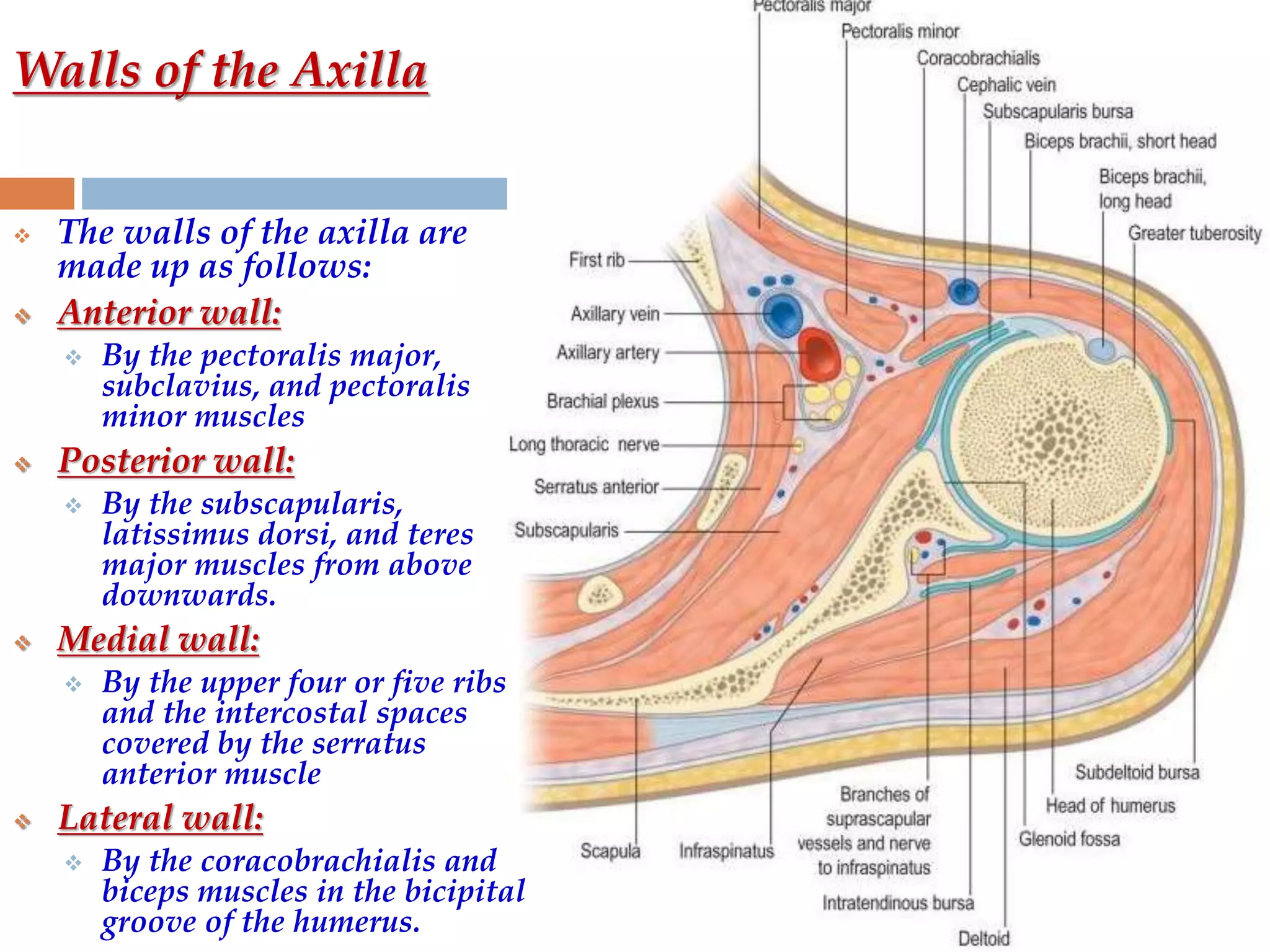
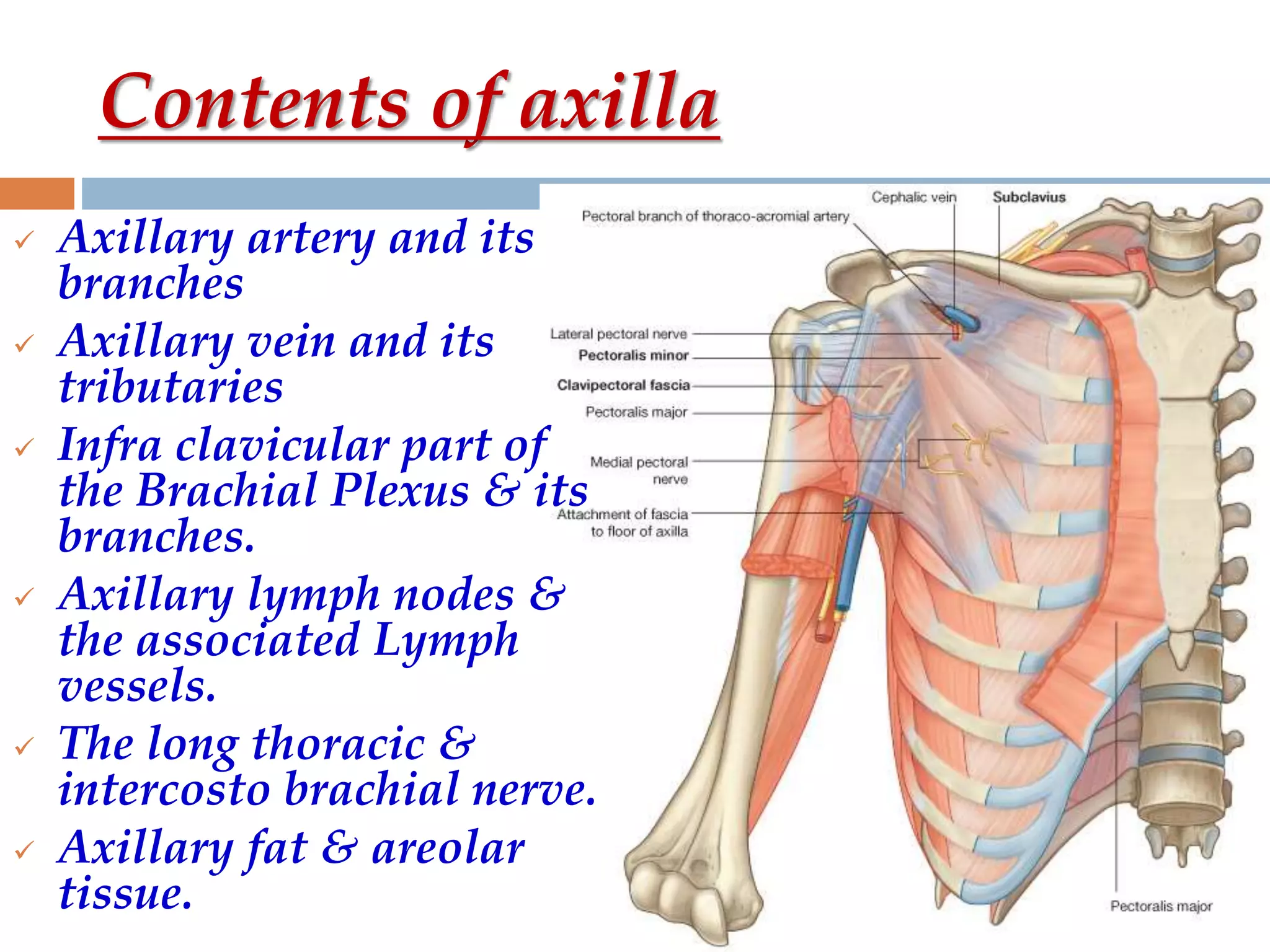
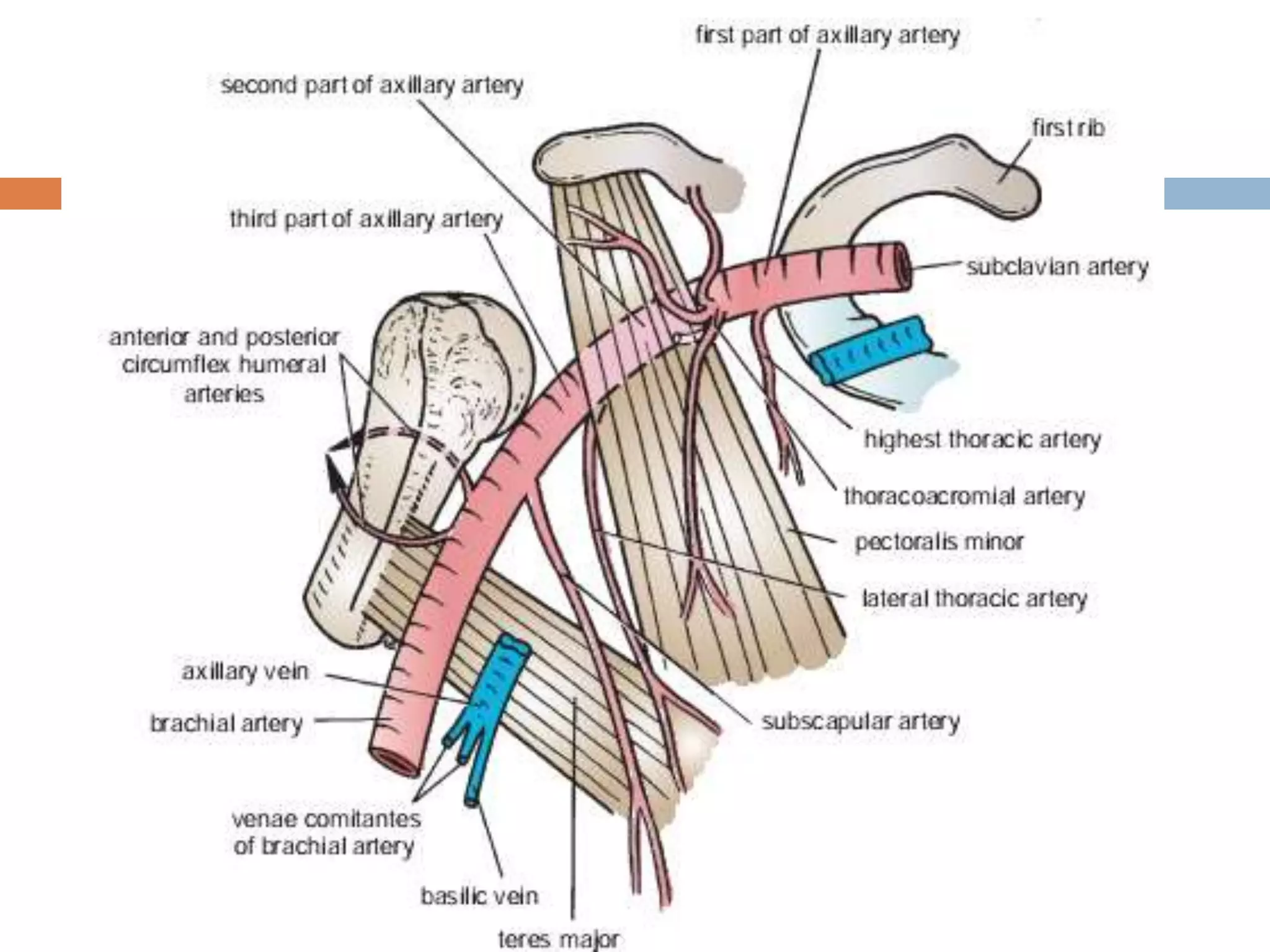
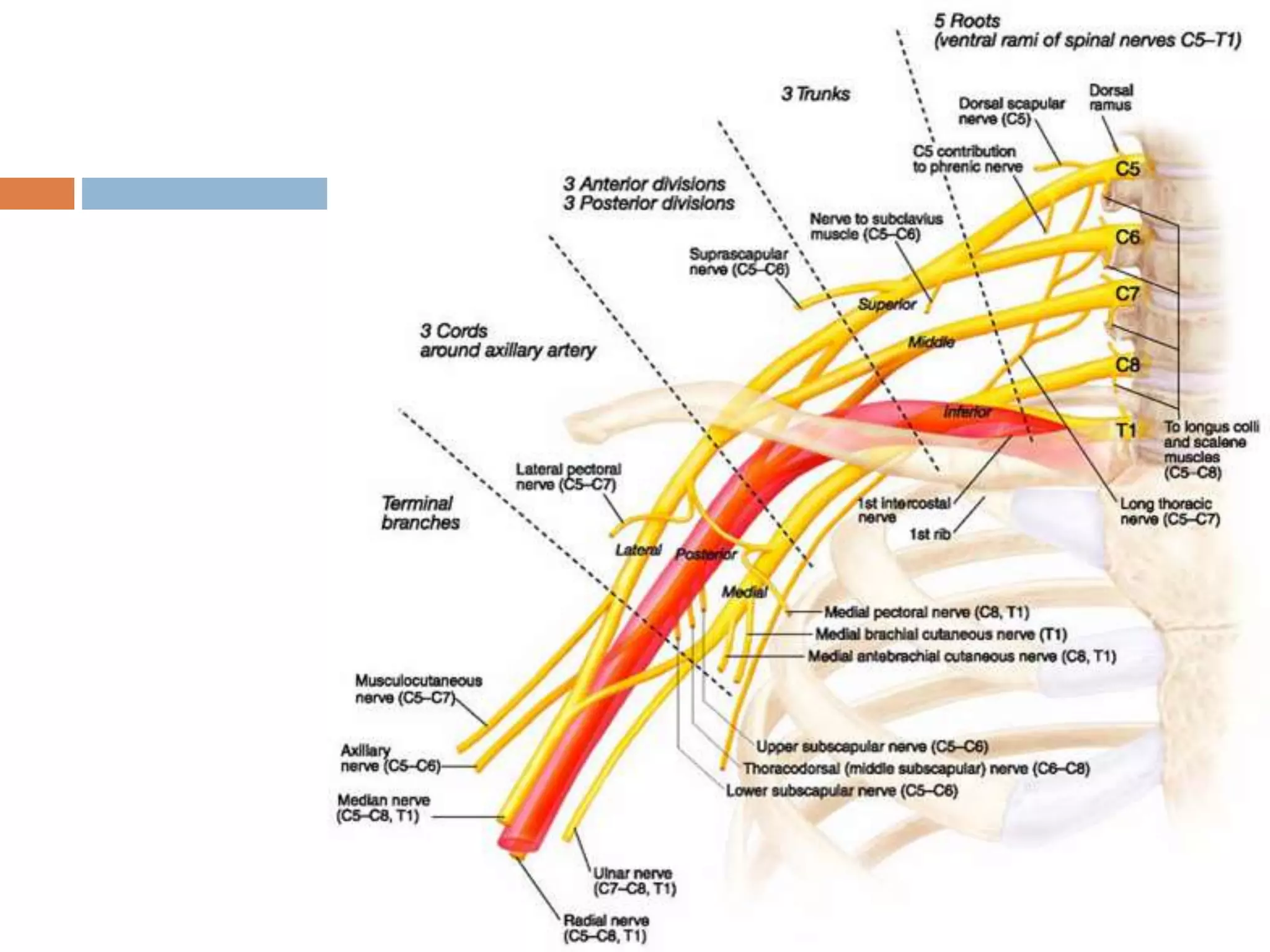
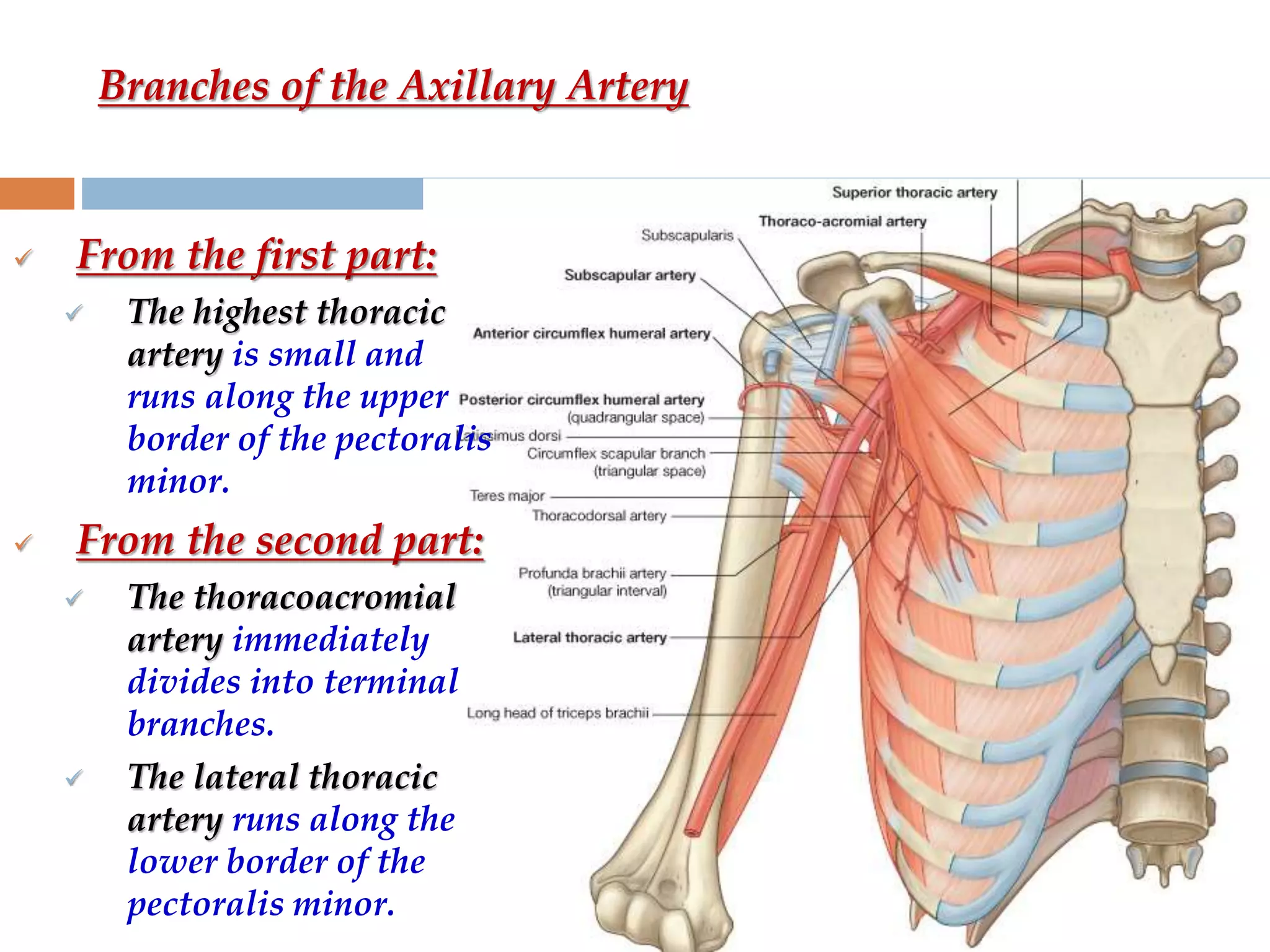
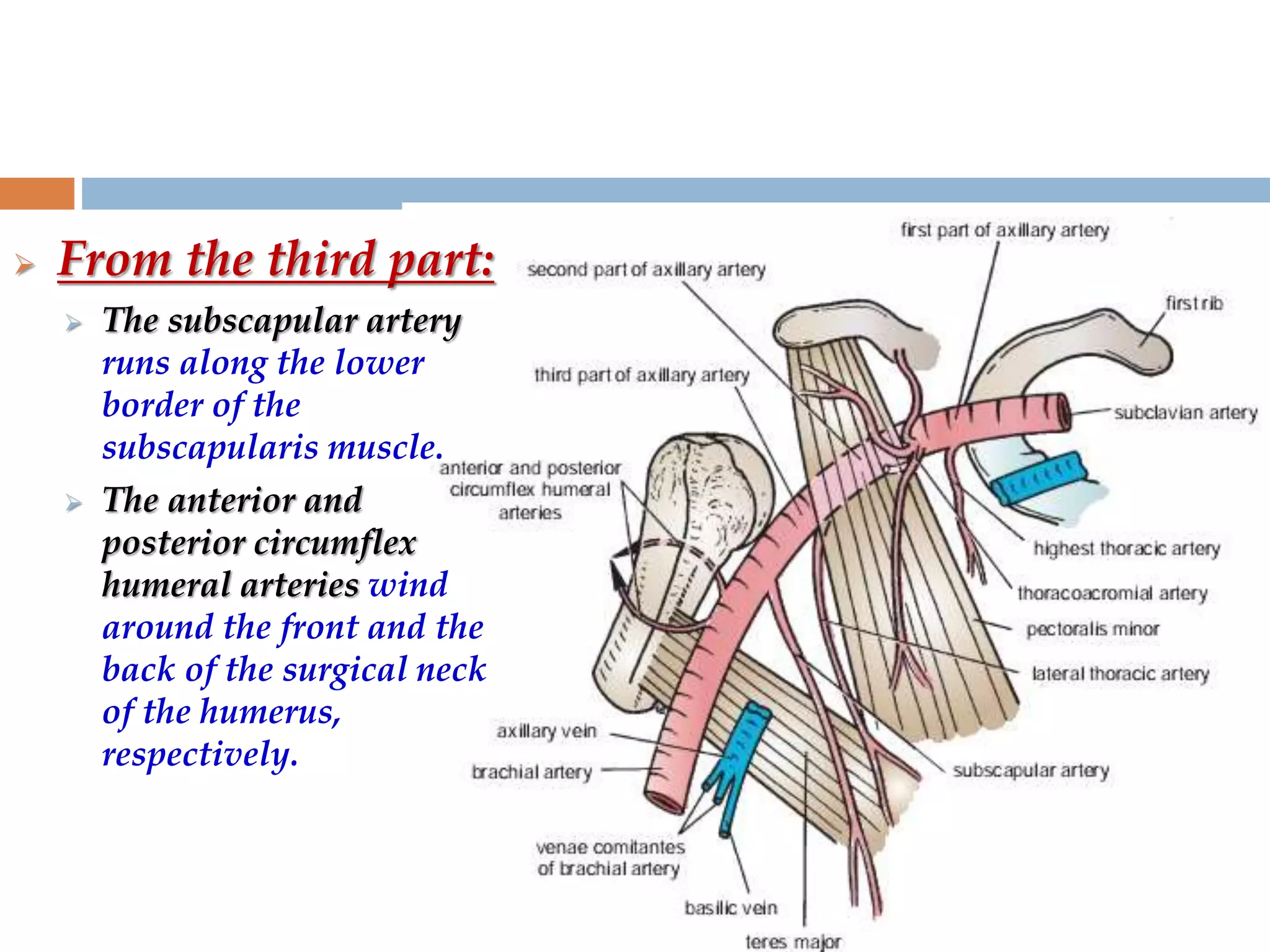
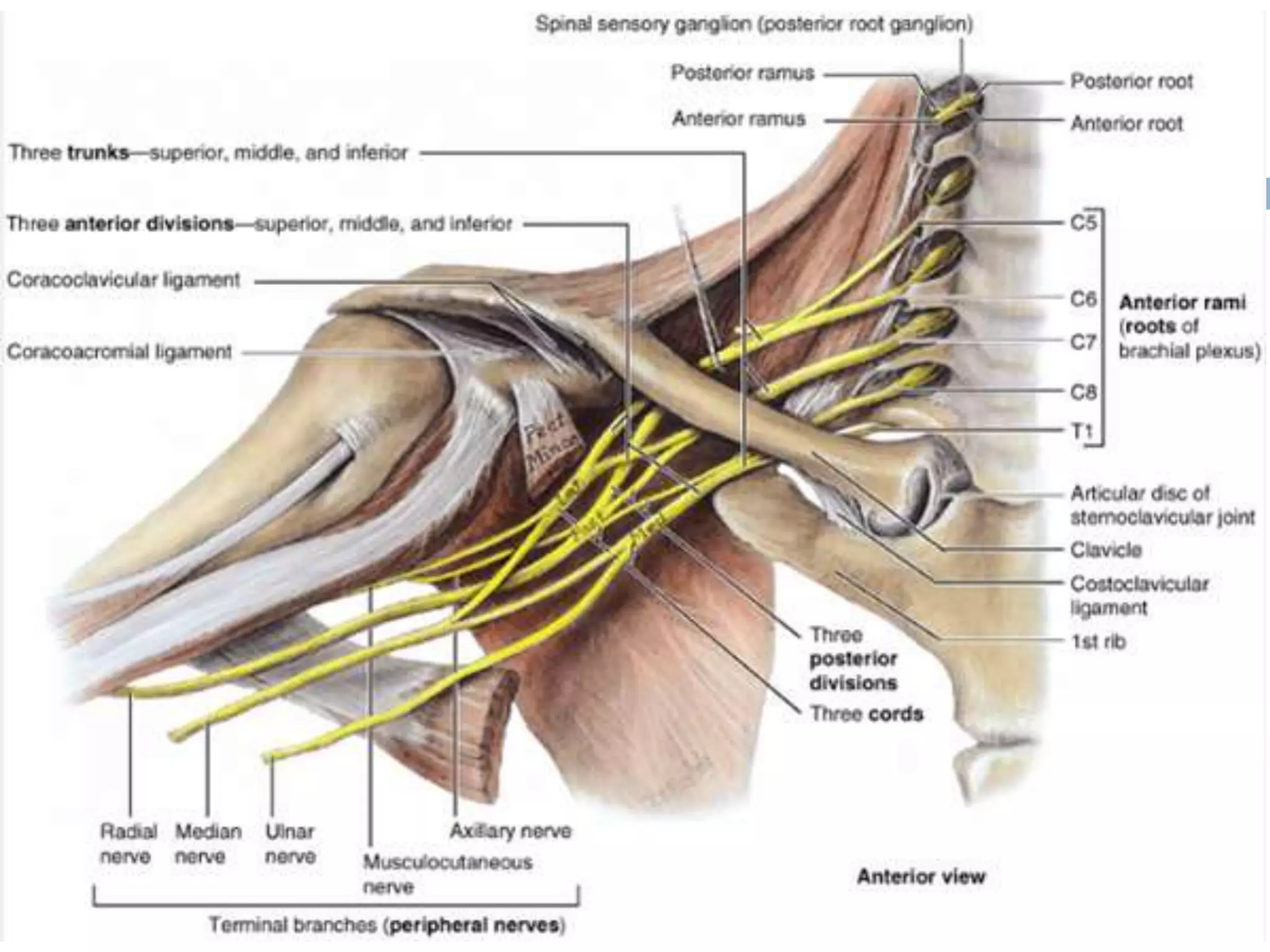
The axilla is a pyramid-shaped space located between the upper arm and chest. It contains nerves, blood vessels, lymph nodes, and fat, and serves as an important passageway. The brachial plexus, formed from cervical and thoracic spinal nerve roots, passes through the axilla, branching into nerves that supply the upper limb. The axillary artery and its branches, including the thoracoacromial, lateral thoracic, and subscapular arteries, also course through the axilla, along with the axillary vein and lymph nodes.




























































![Lecture 25 Intermuscular sapces and axilla [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture25intermuscularsapcesandaxillaautosaved-251110002658-47b36c78-thumbnail.jpg?width=640&height=640&fit=bounds)




























