
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to SLE Presentation
Similar to SLE Presentation (20)
Recently uploaded
Recently uploaded (20)
SLE Presentation
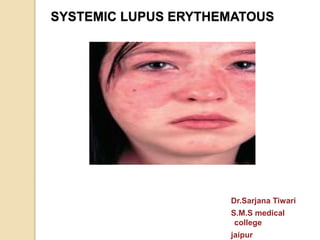
- 1. SYSTEMIC LUPUS ERYTHEMATOUS Dr.Sarjana Tiwari S.M.S medical college jaipur
- 2. CASE: 30 year/Female fever for 3 months multiple joint pains (bilateral knees, wrist and fingers) and swelling for 2 months rash over face and body for 1 month
- 3. History of present illness Fever, mild, intermittent Joint pain, associated with mild swelling and limitation of movement. Rash erythematous, non-itchy, photosensitive No h/o morning stiffness of joints, altered sensorium, any prolonged drug intake or drug allergy, tick infestation in house
- 4. PAST HISTORY : PERSONAL HISTORY FAMILY HISTORY insignificant OCCUPATIONAL HISTORY
- 5. PHYSICAL EXAMINATION: Febrile (100.5 F) HR : 76/min, regular BP : 130/80 mmHg RR : 18/min Pallor:++ Icterus/cyanosis/clubbing/edema - No lymphadenopathy Erythematous rash on face extending over the cheeks and bridge of the nose , sparing the nasolabial folds. Rash over body, erythematous.
- 6. Musculoskeletal- mild swelling and limitation of movements at bilateral proximal inter-phalangeal and bilateral wrist joints. CVS : NAD CNS: NAD RESP SYSTEM: NAD
- 8. INVESTIGATIONS: HEMOGRAM Hb- 8 g/dl WBC- 3.6 ×109/L DLC- N 72%, L 26%, M 2% Platelets – 113 x 109/L Peripheral Smear : no atypical cells ESR – 118 mm
- 9. Renal & Liver Function Tests Blood urea – 23mg/dl Serum Creatinine – 1.5 mg/dl Serum Bilirubin - 0.6 mg/dl Total Protein/ Albumin - 6.5 / 2.8 mg/dl SGOT / SGPT - 23/26
- 10. Urine Examination Protein – 2+ WBC- 10-15 / hpf RBC – 8-10 / hpf Casts – granular cast present 24 hr urinary protein - 1.0 gm / day
- 11. others Chest X ray – WNL X ray Involved joints - WNL
- 12. Revisiting earlier possibilities SLE Rheumatoid arthritis always symmetrical joint invovement erosive arthritis Characteristically has morning stiffness Renal involvement uncommon Dermatomyositis involvement of naso-labial folds myopathy not arthropathy is common no renal or hematological involvement Infective History long No history of tick infestation No leucocytosis or neutrophilia Malignancy no lymphadenopathy No organomegaly Peripheral smear normal
- 13. Rheumatoid factor - Negative ANA- Positive dsDNA – Positive
- 14. Final Diagnosis Characteristic Malar rash Joint symptoms Anemia Deranged renal functions Positive ANA/ ds DNA tests SYSTEMIC LUPUS ERYTHEMATOSIS
- 15. SYSTEMIC LUPUS ERYTHEMATOSUS an autoimmune disease involving multiple organs in which injury is caused mainly by deposition of immune complexes and binding of antibodies to various cells and tissues Acute or insidious in onset.
- 16. EPIDEMIOLOGY: • Female : Male – 9 : 1 • Common in 2nd – 3rd decade • Higher prevalence in blacks and Hispanics
- 17. ETIOLOGY Genetic factors: Higher rate of concordance (25%) in monozygotic twins compared with dizygotic twins(3%) HLA DR2 and DR3 increases risk to 2-5 times Inherited deficiencies of complement (C2,C4,C1q), can be associated. Non MHC genes –TNFα,MBP, IL-6,HSP 70,STAT4,TLR7
- 18. ROLE OF HORMONES IN HUMAN SLE SUSCEPTIBILITY TO SLE DEVELOPMENT: • Use of exogenous estrogens increases risk in women • Certain genes on X chromosome such as TREX-1 plays a role in gender predisposition HORMONES,SLE ACTIVITY AND PROGNOSIS • Disease activity tends to reduce after menopause • Cyclical fluctuation of disease activity in women during the menstrual cycle.
- 19. ENVIRONMENTAL FACTORS Exposure to UV lights: stimulates keratinocytes to produce more IL-1,IL-3,IL-6 and TNFα stimulating B cells to make more antibody. decreases T cell DNA methylation, which may lead to overexpression of LFA(lymphocyte function associated antigen-1).These T cells may then become autoreactive, resulting in autoantibody formation. • Silica dust, cigraette smoke,certain drugs may also increase the risk.
- 20. IMMUNOLOGICAL FACTORS: primarily a disease of immune dysregulation, secondary to a loss of self tolerance. The mediators of SLE are autoantibodies and immune complexes they form with the antigens Defective phagocytosis and clearing of immune complexes, leads to their persistence the increased autoantibody production and persistence is not downregulated appropriately by anti-idiotypic antibodies, by CD 4+regulatory Tcells or by CD 8+ suppressor T cells. Some immune complexes particularly those containing DNA or RNA activate the innate immune system viaTLR9 or TLR7 respectively. Dendritic cells are activated and release type 1 interferons and TNFα, T cells release IFN-gamma, IL 6, IL 10, while NK Cells and T Cells fail to release adequate quantities of TGF- beta, thus favouring continued autoantibody formation.
- 24. Constitutional symptoms non-specific symptoms - Fatigue - Fever - Weight Loss
- 26. The large, friable vegetations are denoted by arrows in infective endocarditis INFECTIVE ENDOCARDITIS NON BACTERIAL ENDOCARDITIS Nearly complete row of thrombotic vegetations along the line of closure of the mitral valve leaflets
- 30. EVALUATION FOR SUSPECTED SLE The diagnosis of SLE must be based on proper constellation of clinical findings and laboratory evidence.
- 31. INITIAL TESTS: Full blood count with Differentials: May reveal leukopenia, mild anemia and thrombocytopenia ESR and CRP Levels are elevated However the level of ESR elevation may show a discrepency relative to normal CRP level in SLE flares Clotting tests A prolongation of the partial thrombomboplastin time would suggest the presence of lupus anticoagulant and should prompt checking of antiphospholipid antibodies.
- 32. Blood culture / Urine culture To screen for infection Urinalysis with microscopy May reveal proteinuria, hematuria and/or cellular casts Serum urea and creatinine Elevated level may be seen in renal dysfunction Complement levels C3 and C4 levels are often depressed in active SLE as a result of consumption by immune complex induced inflammation.
- 33. ANAASSAY The ANA assay is an ideal screening test because of its sensitivity (95%) and simplicity. Technique to detect ANA: The indirect immunofluorescence test is most widely used assay for detection of ANA Titre>1:40 is considered positive
- 35. OTHER AUTOANTIBODIES: Antibodies prevelance Anti-ds DNA 70% Anti-Sm antigen 30% Anti-Ro/SSA 30% Anti-La/SSB 20% Anti-U1RNP 25% Antiribosomal P protein 10% Anti –ds DNA and Anti-Sm antigen is highly specific for SLE
- 36. LE TEST Lupus erythematosus (LE) cell test was once performed to diagnose SLE but has now been replaced by ANA test. LE cell is any phagocytic leukocyte (neutrophil or macrophage) that has engulfed the denatured nucleus of an injured cell. A lupus erythematosus (LE) cell test is considered positive when approximately 2%-30% of the cells seen on the slide in the neutrophil count are LE cells.
- 37. LE CELL:
- 38. IMAGING Diagnostic imaging may be valuable, but is not routinely obtained unless indicated by the presence of symptoms, clinical findings, or laboratory abnormalities. Examples include: Plain radiographs of swollen joints. Unlike affected joints in RA, erosions are observed infrequently in SLE Renal ultrasonography to assess kidney size and to rule out urinary tract obstruction when there is evidence of renal impairment Chest radiography (eg, for suspected pleural effusion, interstitial lung disease, cardiomegaly).
- 39. Echocardiography suspected pericardial involvement, to assess for a source of emboli, or noninvasive estimation of pulmonary artery pressure; and for evaluation of suspected valvular lesions, such as verrucae, etc Computed tomography (CT) Evaluating abdominal pain, suspected pancreatitis, interstitial lung disease, etc Magnetic resonance imaging (MRI) Evaluating focal neurologic deficits or cognitive dysfunction
- 40. BIOPSY: • RENAL BIOPSY: The 2012 American College of Rheumatology (ACR) guidelines for lupus nephritis recommend renal biopsy for all cases of active , previously untreated lupus nephritis, unless contraindicated. Renal biopsy is used to: confirm the presence of lupus nephritis; to aid in classification of systemic lupus erythematous (SLE) nephritis based on the International Society of Nephrology/Renal Pathology Society (ISN/RPS) classification to guide therapeutic decisions.
- 41. INDICATIONS OF RENAL BIOPSY Increasing serum creatinine in the absence of strong evidence for another etiology (eg, sepsis, hypovolemia, medication) Proteinuria > 1.0 g per 24 hours, as confirmed by 24-hour urine specimens or spot protein/spot creatinine ratios Proteinuria ≥ 0.5 g per 24 hours, along with either (1) hematuria ( ≥5 RBCs/hpf ) or (2) cellular casts, as confirmed by a minimum of 2 tests within a short period and in the absence of alternative causes
- 43. NORMAL GLOMERULUS MESENGIAL PROLIFERATIVE GN . Light micrograph of a normal glomerulus. There are only 1 or 2 cells per capillary tuft, the capillary lumens are open, the thickness of the glomerular capillary wall (long arrow) is similar to that of the tubular basement membranes (short arrow), and the mesangial cells and mesangial matrix are located in the central or stalk regions of the tuft (arrows). Light micrograph of a mesangial glomerulonephritis showing segmental areas of increased mesangial matrix and cellularity (arrows).
- 44. Light micrograph showing a membranoproliferative pattern in lupus nephritis, characterized by areas of cellular proliferation (long arrows) and by thickening of the glomerular capillary wall (due to immune deposits) that may be prominent enough to form a "wire-loop" (short arrows). Although proliferative changes can be focal (affecting less than 50 percent of glomeruli), disease of this severity is usually diffuse MEMBRANOPROLIFERATIVE GN
- 45. Kidney biopsy from a patient with diffuse proliferative lupus nephritis showing, on immunofluorescence microscopy, massive, lumpy deposits of IgG
- 46. Light micrograph of membranous lupus nephritis. The changes are similar to those in any form of membranous nephropathy with diffuse thickening of the glomerular capillary wall being the major abnormality (short arrows). Focal areas of mesangial expansion and hypercellularity (long arrows) are the only findings suggestive of an underlying disease such as lupus, although they can also be seen in idiopathic membranous nephropathy. MEMBRANOUS LUPUS NEPHRITIS
- 47. Electron micrograph of a normal glomerular capillary loop showing the fenestrated endothelial cell (Endo), the glomerular basement membrane (GBM), and the epithelial cells with its interdigitating foot processes (arrow). The GBM is thin, and no electron-dense deposits are present. Two normal platelets are seen in the capillary lumen. Electron micrograph of membranous lupus nephritis. The subepithelial immune deposits (D) are characteristic of any form of membranous nephropathy, but the intraendothelial tubuloreticular inclusions (arrow) strongly suggest underlying lupus.
- 48. Skin biopsies: Histologically the involved areas shows: vacuolar degeneration of the basal layer of epidermis In the dermis there is edema and perivascular inflammation.
- 50. POOR PROGNOSTIC INDICATORS Male sex Black racial background Young age at onset of nephritis Hypertension Nephrotic syndrome Elevated creatinine level(>3 mg/dl) at presentation Renal biopsy findings showing diffuse lupus nephritis
- 51. Goals of therapy – Stop and reverse ongoing organ inflammation – Prevent or limit irreversible end-organ damage the average 10 year survival rates >90%, with newer immunosuppressive therapies
- 52. Treatement; Non pharmocological treatement: Sun protection: avoid sun exposure and use sunscreens. Pharmocological treatement: Hydroxychloroquine/chloroquine Prednisolone Immunosuppresive drugs like azathioprine,methotrexate,cyclophosphamide Belimumab:B – lymphocyte stimulator specific inhibitor
- 54. CONDITION DIFFERENTIATING SIGNS/SYMPTOMS DIFFERENTIATING TESTS Rheumatoid arthritis • May be difficult to differentiate clinically • Patients with SLE frequently presents with pattern similar to arthritis, although it tends to be less symmetrical • In RA Joint x-rays demonstrate symmetrical, erosive arthritis. • Serologic abnormalities such as anti-cyclic citrullinated peptides (CCP) suggests RA, Systemic sclerosis • Raynaud's phenomenon is present in almost all patients • Patients with SLE often have Raynaud's phenomenon as well, but these tend not to ulcerate compared with patients with systemic sclerosis. • systemic sclerosis have characteristic sclerodactyly and calcinosis, not present in SLE. • Auto-antibodies: positive anti-centromere antibodies (limited cutaneous systemic sclerosis) or anti- topoisomerase 1 (Scl- 70) antibodies (diffuse cutaneous systemic sclerosis).
- 55. Sjögren’s syndrome • patients with Sjögren’s syndrome should have objective signs of keratoconjunctivitis sicca and xerostomia • salivary gland biopsy is essential for diagnosis of sjogren’s syndrome.The key histologic feature is a focal collection or collections of tightly aggregated lymphocytes, which are typically periductal. • anti-SSA, anti-SSB are present in 70-95% of patients Mixed connective tissue disorders • MCTD is characterised by a combination of manifestations similar to those in SLE, systemic sclerosis, and myositis. Difficult to differentiate clinically. Auto-antibodies: positive anti-RNP antibodies are specific to MCTD. Patients with MCTD tend to lack other antibodies such as anti-Sm, anti-Ro, anti- La, and anti-dsDNA.
- 56. Dermatomyositis (DM) and polymyositis (PM) DM and PM demonstrate more symetrical proximal muscle weakness Patients with DM may have characteristic skin findings including Gottron’s papules, a heliotrope eruption and poikiloderma (including the shawl and V signs). The specific anti-Jo-1 antibody can help differentiate the diagnosis with SLE. malignancies • Leukemia or myelodysplastic syndromes may present with hematologic and constitutional symptoms similar to those observed in SLE. • Patients with lymphoma also typically have additional findings such as splenomegaly, lymphadenopathy, or increased lactate dehydrogenase (LDH) levels. monoclonal expansion of B and T cells (as assessed by immunophenotyping), monocytosis, or macrocytosis can distinguish these malignancies from SLE.
- 57. Behçet’s disease • Oral aphthae are present in almost all patients with Behçet’s disease, and may be observed in patients with SLE. • Other overlapping features include inflammatory eye disease, neurologic disease, vascular disease, and arthritis • Behcet’s commonly occurs in males patients with Behçet’s are ANA-negative. Also, vascular involvement of any size (small, medium, large) is more commonly a feature of Behçet’s disease rather than SLE. Drug induced lupus • The clinical symptoms are mild and reversable after discontinue medication. • CNS and kidney are unusually involved. The antihistone antibodies differentiate the diagnosis with SLE.
- 58. THANK YOU
Editor's Notes
- deposition of immonoglobulins and complements along dermoepidermal junction