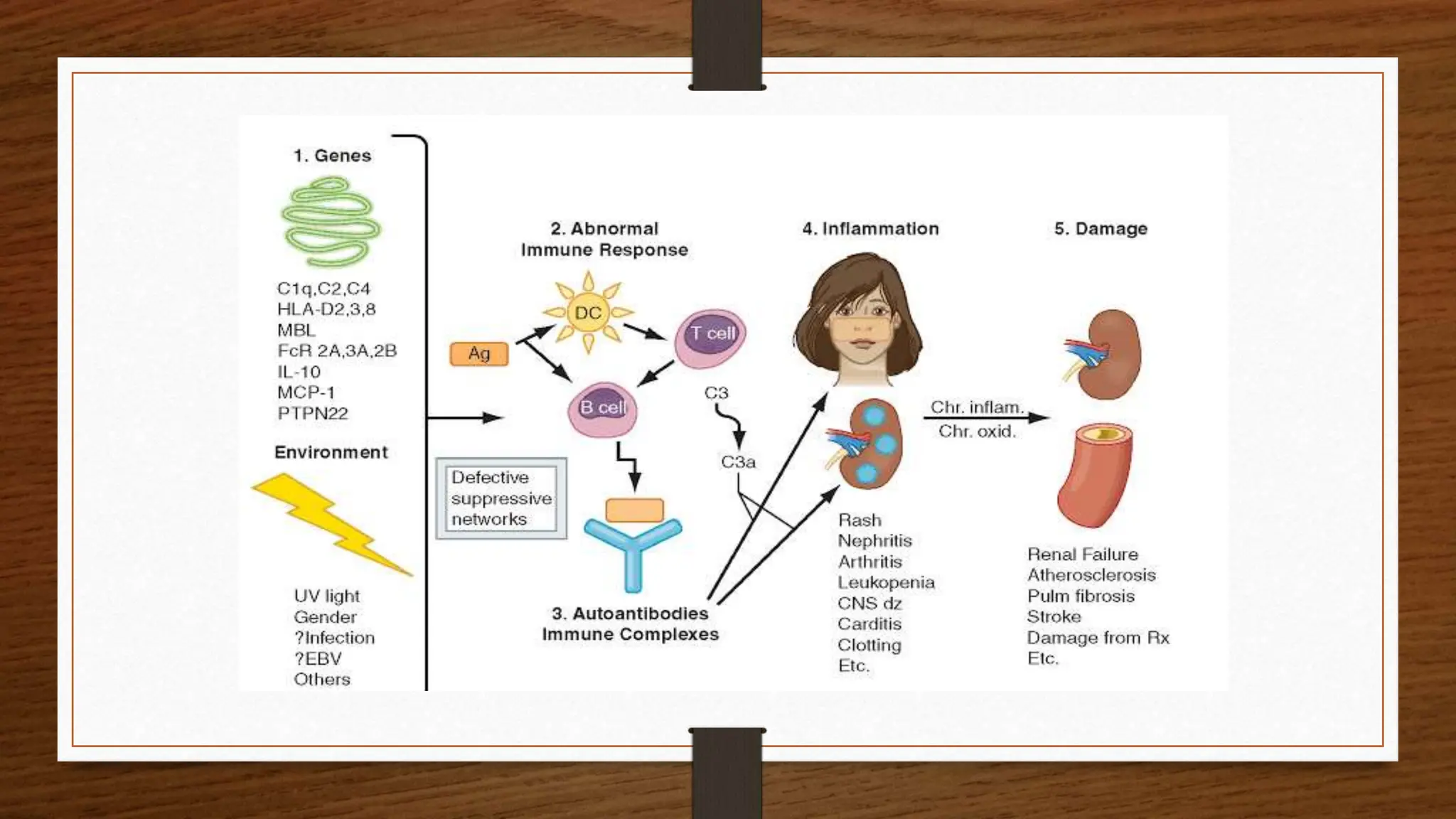
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by the production of autoantibodies that result in damage to multiple organs, primarily affecting young women between ages 20-30. The prevalence is notably higher among African-American and Afro-Caribbean women, with risk factors including family history, smoking, and infections. Diagnosis involves clinical presentation and various lab tests, while treatment options range from immunosuppressants to corticosteroids depending on the severity and specific symptoms.