Downloaded 39 times

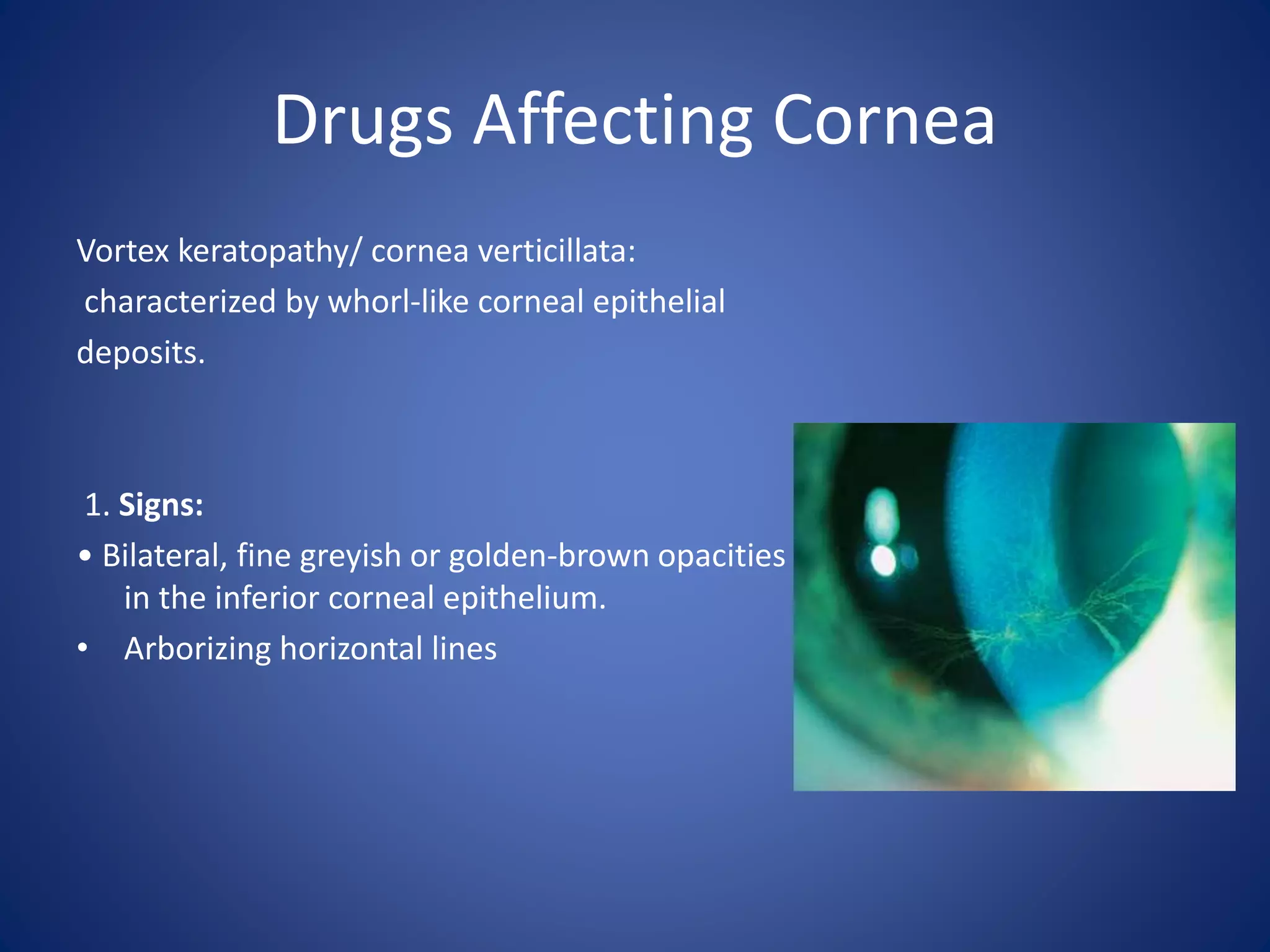
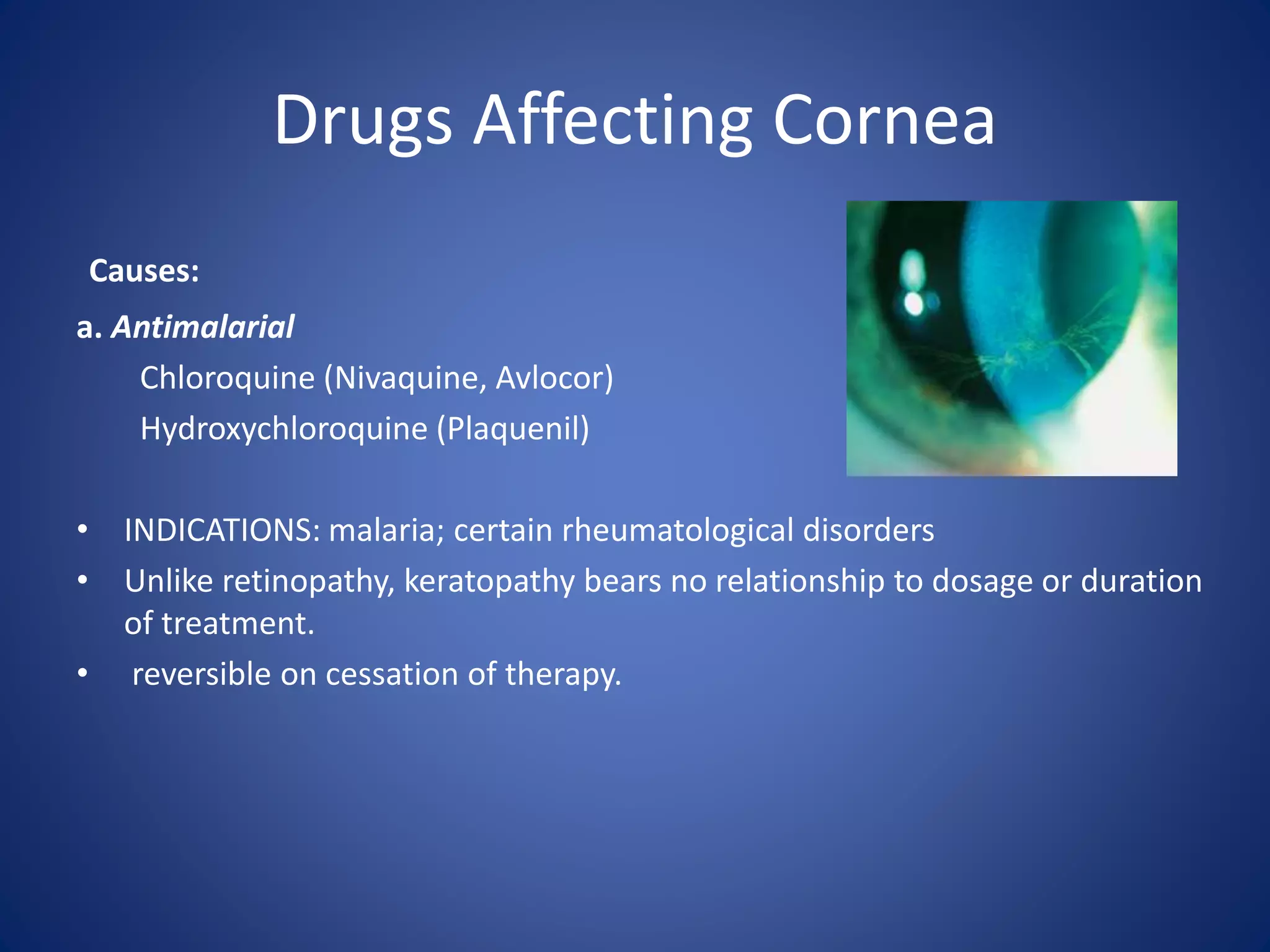
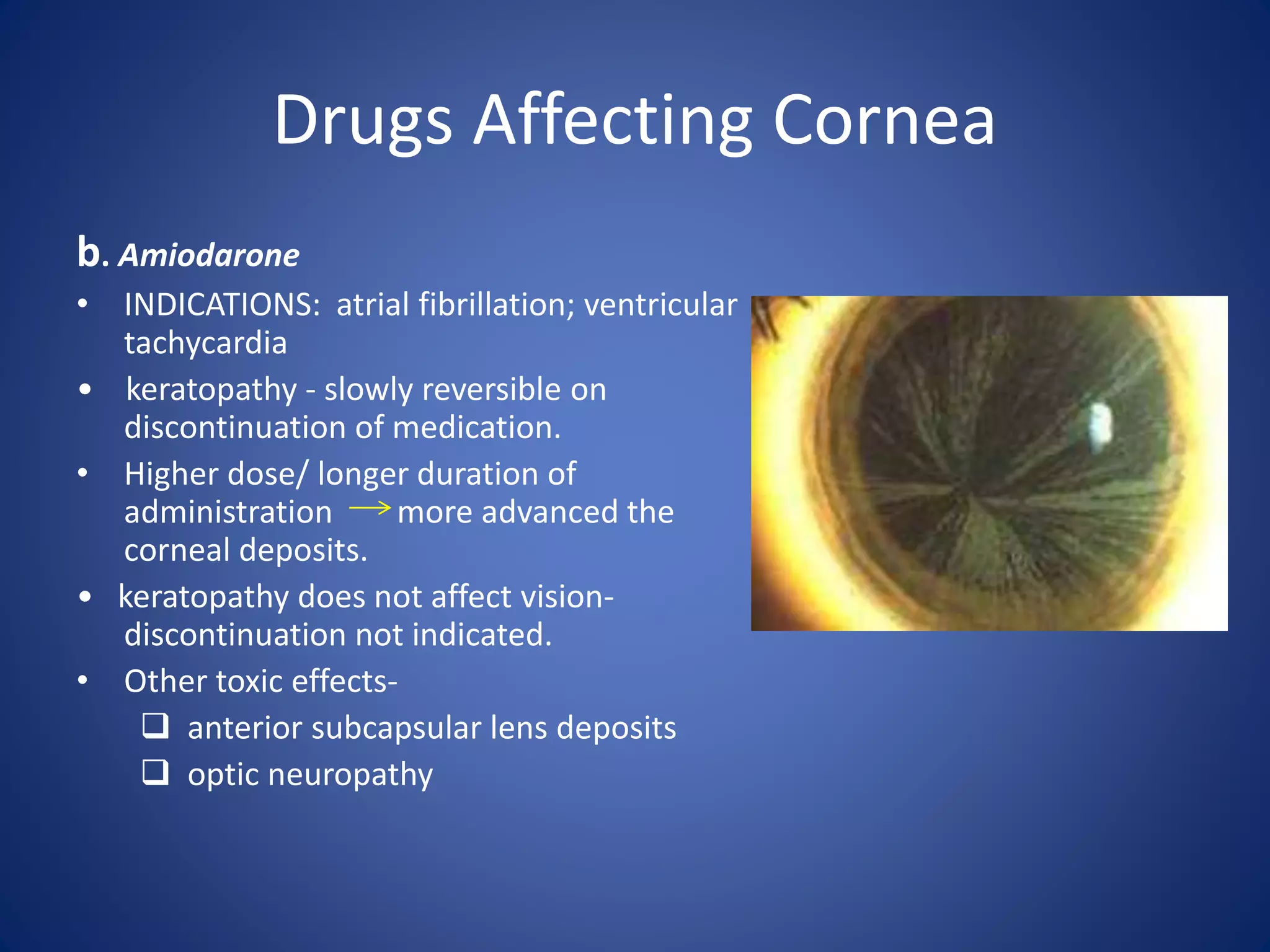
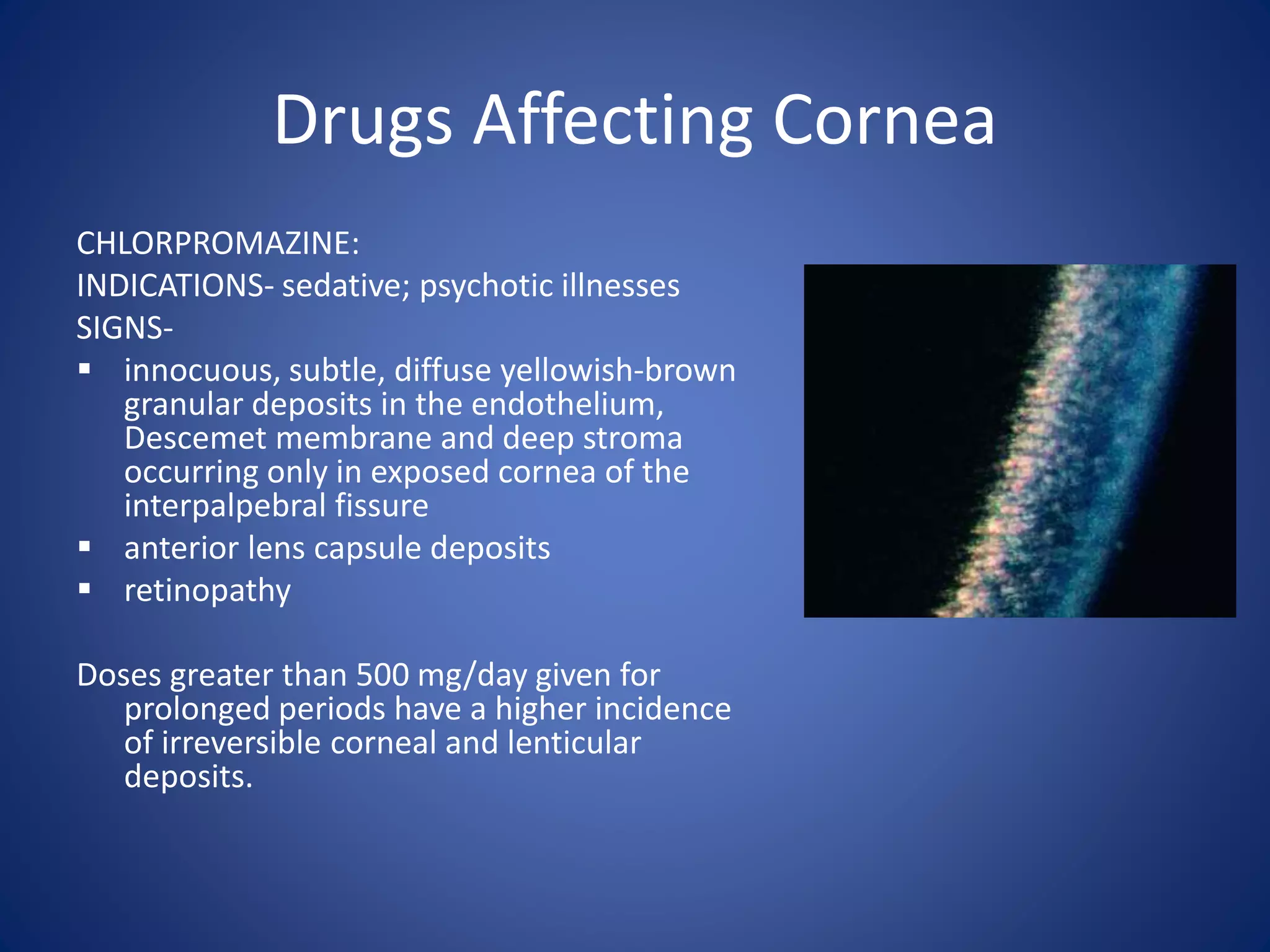
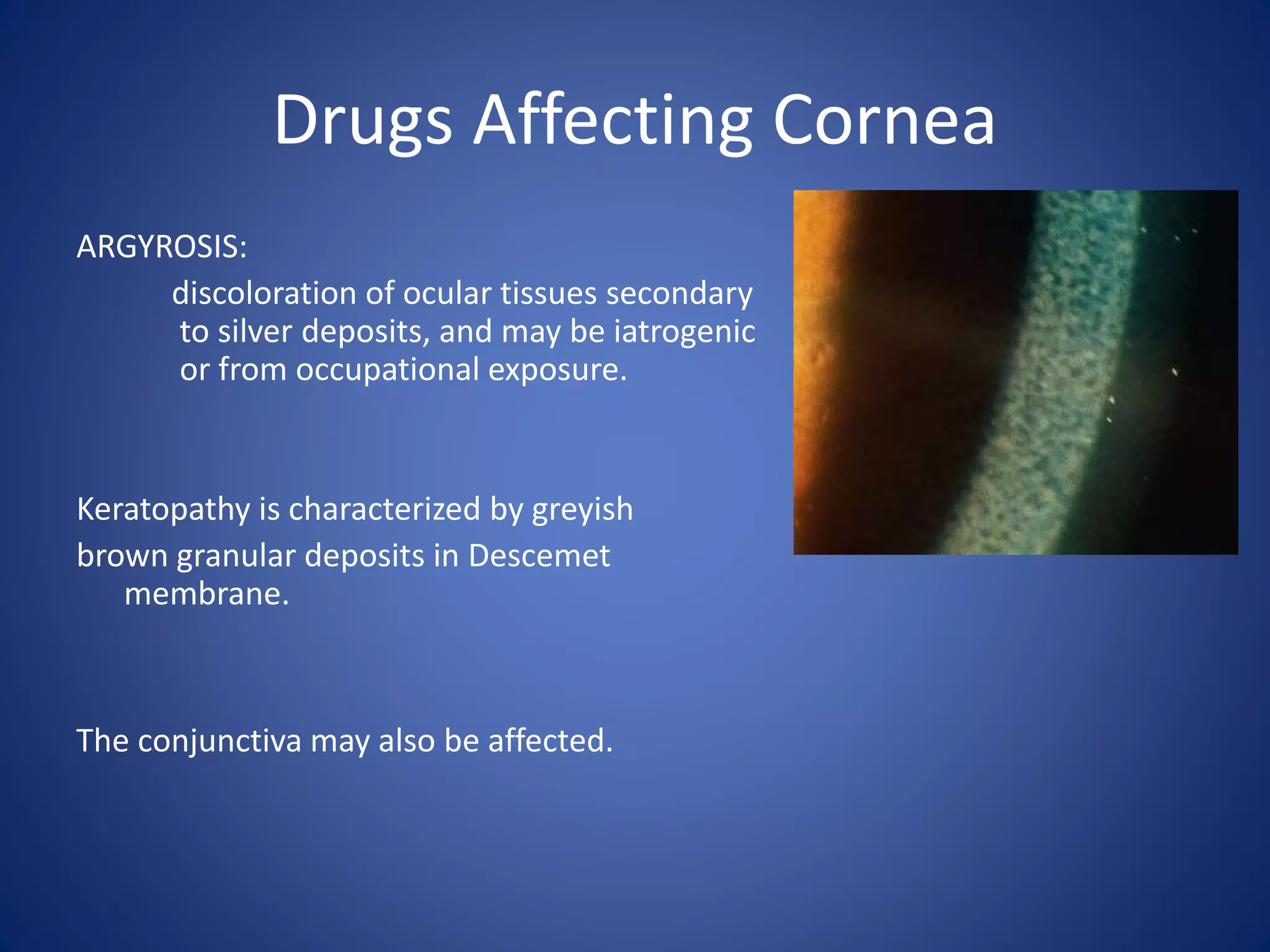
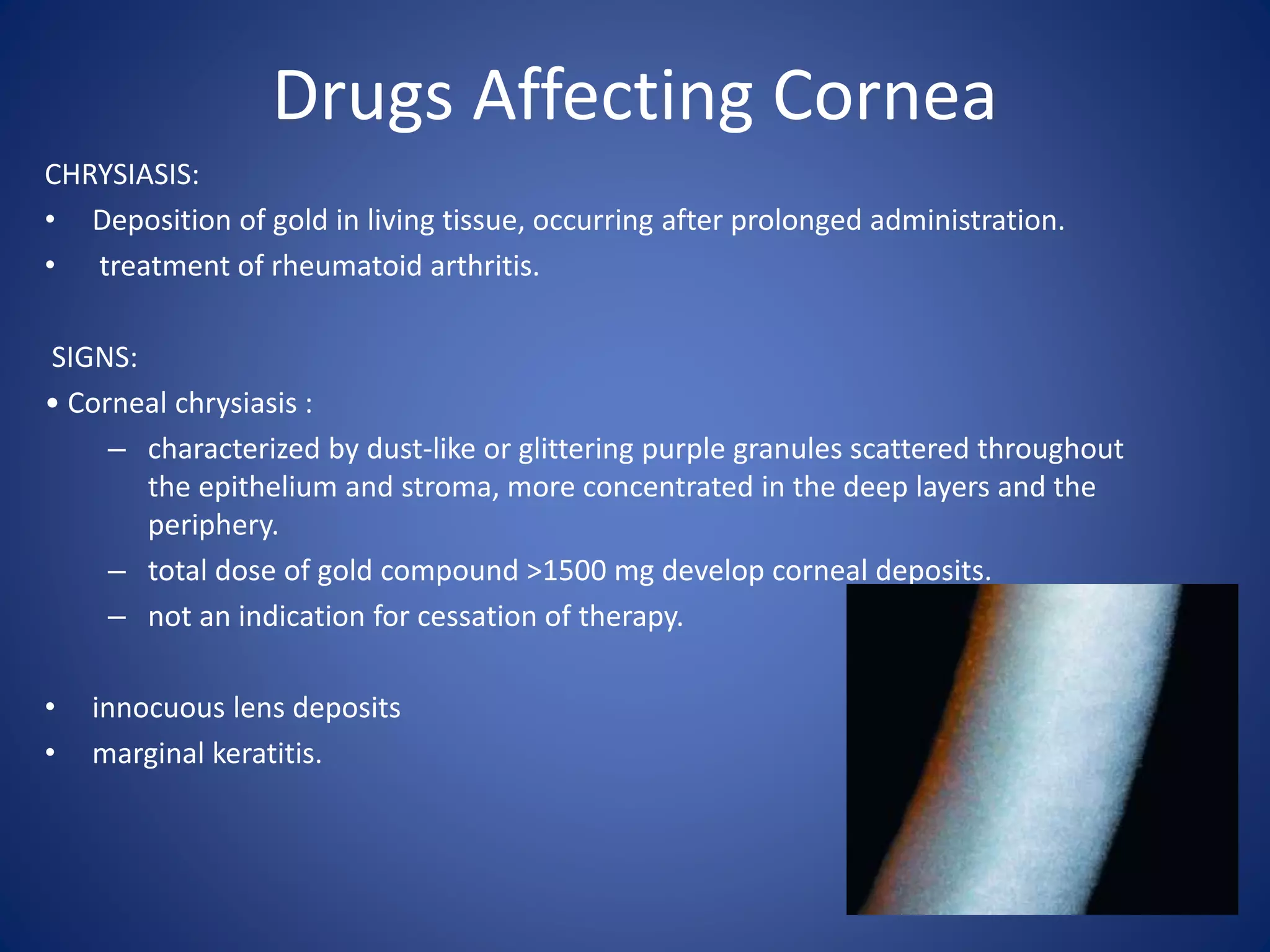

Vortex keratopathy, characterized by whorl-like corneal epithelial deposits, can be caused by long-term use of antimalarial drugs like chloroquine and hydroxychloroquine. Amiodarone, used to treat arrhythmias, can also cause slowly reversible corneal deposits. Prolonged use of chlorpromazine above 500 mg daily is linked to irreversible corneal and lens deposits. Prolonged administration of medications containing silver or gold can lead to gray-brown or purple corneal deposits respectively, through argyrosis or chrysiasis.

































































































