Anatomy
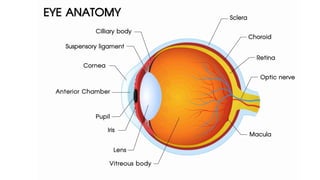
Globe of eyeconsists of 3 layers:
1. Cornea-sclera
2. Choroid-iris
3. Retina
5.
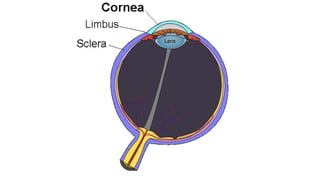
Cornea-sclera
- Transparent structure,continuation of the conjunctiva over the
cornea present in the anterior part of the eyeball
- Sclera is the outermost layer of the eyeball
7.
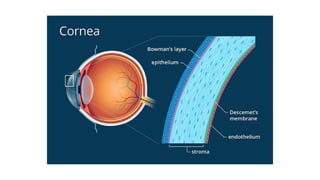
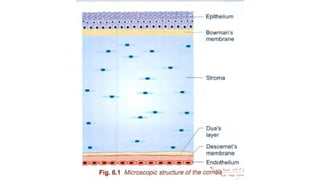
Anatomy of theCornea
The cornea is the transparent, avascular outermost layer of the
eye, playing a key role in focusing light. It consists of six layers:
1. Epithelium:
○ Outermost layer, provides barrier and smooth refractive
surface.
○ Regenerates rapidly after minor injuries.
2. Bowman’s Layer:
○ Acellular, collagen-rich layer beneath the epithelium.
8.
3. Stroma:
○ Makesup ~90% of corneal thickness.
○ Contains collagen fibrils and keratocytes.
○ Maintains corneal transparency through regular fibril
arrangement and dehydration.
4. Pre-Descemet’s membrane(Dua’s layer)
5. Descemet’s Membrane:
○ Basement membrane of the endothelium.
○ Thickens with age and can regenerate.
9.
6. Endothelium:
○ Singlelayer of cells on the inner surface.
○ Maintains corneal dehydration via active ion transport
(Na /K ATPase).
⁺ ⁺
○ Non-regenerative; damage leads to corneal edema.
12.
Blood supply:
- Itis an avascular structure
Nerve supply:
- Supplied by long ciliary nerves which are branches
of nasociliary nerve from ophthalmic division of
trigeminal nerve
- 3 plexuses: stromal, subepithelial and intraepithelial
13.
Functions
- Acts asa major refracting medium
- Protects intraocular contents
Corneal degenerations
- Conditionsin which normal cells undergo some degenerative
changes under the influence of age or other pathological
conditions
- They can be either unilateral or bilateral
- Non-familial
Types of CornealDegeneration:
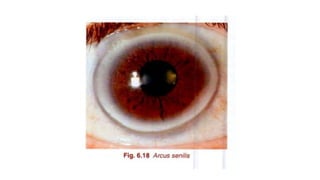
1. Arcus Senilis (Gerontoxon)
● Site: Peripheral corneal stroma.
● Features: Grayish-white arc (lipid deposits), usually bilateral.
● Cause: Age-related lipid metabolism changes.
● Effect on vision: Usually none.
20.
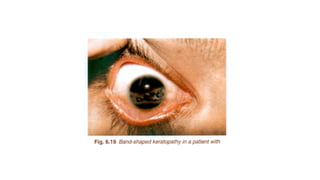
2. Band Keratopathy
●Site: Bowman's layer and superficial stroma.
● Features: Calcium deposition appearing as a horizontal band
across the cornea.
● Associated with: Chronic uveitis, hypercalcemia, renal failure.
● Effect: May impair vision if it involves the visual axis.
Corneal dystrophy
- Groupof disorders characterised by non-inflammatory,
inherited, bilateral opacity of cornea with no vascularisation
- Inborn defect
- Bilateral dystrophy
- No associated systemic disease
- Manifests usually by 1st to 2nd decade of life
30.
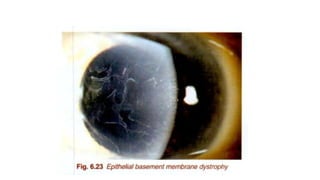
Classification of cornealdystrophies:
- Epithelial and subepithelial dystrophies
- Bowman layer dystrophies
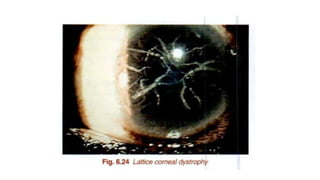
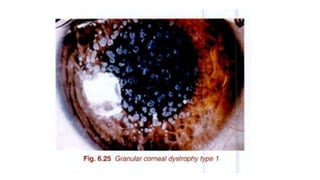
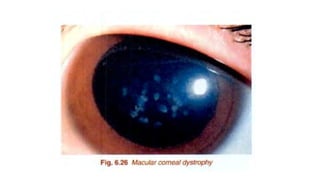
- Stromal dystrophies
- Descemet membrane and endothelial dystrophies
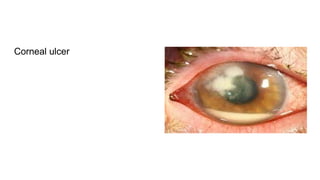
Corneal ulcer
- Itis a discontinuation in normal epithelial surface of
cornea
- demonstrated by staining with 1% sodium fluorescein dye
and viewed with cobalt blue filter light .
Corneal Abrasion or Erosion: the epithelial defect, if
superficial without inflammation
Corneal Ulcer: epithelial defect with inflammation in the
surrounding area. May be infective or sterile .
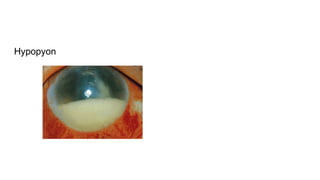
Hypopyon
Definition: hypopyon isthe accumulation of pus resulting from
suppurative infection inferiorly in the anterior chamber
● Consists of neutrophils which accumulate in the lower angle of
anterior chamber and eventually become enmeshed in a
network of fibrin .
● It is seen in severe corneal ulcers as a collection of pus in the
anterior chamber
Risk Factors
Contact LensUse (most common)
● Poor hygiene (e.g., rinsing with tap water)
● Wearing lenses while swimming, showering, or using hot tubs
● Improper disinfection/storage
Corneal Trauma: Especially with exposure to contaminated water
or soil
Symptoms
● Severe eyepain (often disproportionate to clinical findings)
● Eye redness
● Blurred vision
● Photophobia (light sensitivity)
● Excessive tearing
● Sensation of something in the eye (foreign body sensation)
● Ring infiltrate in the cornea (late-stage, pathognomonic)
● Ulceration and stromal inflammation
54.
Diagnosis
Clinical Evaluation
● Historytaking, especially contact lens usage and water
exposure
● Slit-lamp examination
Laboratory Tests
1. Corneal scraping
○ Microscopic examination with stains (e.g., calcofluor white,
Giemsa)
○ Culture on non-nutrient agar with E. coli overlay
55.
2. Confocal microscopy
○shows cysts and trophozoites in the cornea
3. PCR (Polymerase Chain Reaction)
4. Immunofluorescence assays
56.
Treatment
Medical Therapy
● Topicalagents:
○ Biguanides (e.g. PHMB 0.02%, chlorhexidine 0.02%)
○ Diamidines (e.g. hexamidine)
● Combination therapy of biguanide + diamidine is preferred
● Dosing initially every hour for several days to weeks
57.
● Cycloplegics forpain control
● Oral antifungals (e.g., itraconazole, voriconazole) in severe
cases
Surgical Options
● Penetrating keratoplasty (corneal transplant) in refractory or
advanced cases with corneal perforation or scarring
Mycotic Keratitis
Mycotic keratitis,also known as fungal keratitis
Infection of the cornea caused by fungal organisms
Significant cause of corneal blindness
60.
Causative Agents
Fungal keratitiscan be caused by filamentous fungi and yeasts.
a) Filamentous fungi:
● Fusarium
● Aspergillus
● Curvularia
b) Yeasts:
● Candida albicans and other Candida species
61.
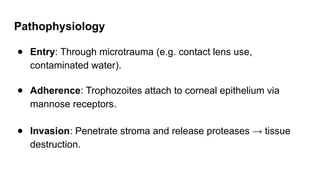
Pathogenesis
Corneal Injury orPredisposing Factor
● Entry often follows trauma with vegetative matter, contact
lens use, ocular surgery, or prolonged steroid use.
Adherence and Penetration
● Fungal spores adhere to damaged epithelium.
● Filamentous fungi penetrate the corneal stroma by extending
hyphae, causing mechanical and enzymatic damage.
62.
Immune Response
● Hostmounts an inflammatory response involving neutrophils
and macrophages.
● This results in corneal ulceration, stromal necrosis, and
possible hypopyon.
Progression
● The infection can progress to deep stromal involvement and
corneal perforation if not treated promptly.
63.
Symptoms
Gradual onset ofsymptoms:
● Eye pain
● Redness
● Foreign body sensation
● Photophobia
● Blurry vision
● Watery or mucopurulent discharge
● White or grayish corneal ulcer with feathery borders
● Satellite lesions may be present
● Hypopyon (pus in the anterior chamber) in advanced cases
64.
Diagnosis
a) Clinical Examination
●Slit-lamp findings: Dry-looking ulcer with feathery margins,
satellite lesions, endothelial plaque, and possible hypopyon.
b) Laboratory Tests
● Corneal scraping:
○ KOH wet mount – reveals branching hyphae (filamentous
fungi)
65.
○ Gram stain– useful for Candida
○ Culture on Sabouraud Dextrose Agar (SDA)
● Confocal microscopy – can visualize fungal filaments in vivo
● PCR – for species identification (advanced centers)
66.
Treatment
a) Topical AntifungalTherapy
● Natamycin 5% – first-line treatment for filamentous fungi
(Fusarium, Aspergillus)
● Amphotericin B 0.15% – effective for yeasts (Candida) and
some filamentous fungi
● Voriconazole 1% – broad-spectrum, especially useful in
resistant or deep infections
67.
b) Oral AntifungalTherapy
● Used in severe or deep stromal infections:
○ Voriconazole, Itraconazole, Fluconazole (especially for
Candida)
c) Adjunctive Therapy
● Cycloplegics to relieve ciliary spasm and pain
● Avoid corticosteroids
d) Surgical Intervention
● Therapeutic penetrating keratoplasty
Causative Agent
Adenovirus –serotypes 8, 19, and 37
Part of the adenovirus group D
Spread through:
● Direct contact with eye secretions
● Contaminated hands, towels, instruments (e.g., tonometers)
● Swimming pools and ophthalmic clinics
71.
Incubation and Transmission
Incubationperiod: 5–12 days
Highly contagious, even before symptoms begin
Can spread rapidly in hospitals, schools, or offices
72.
Symptoms
● Redness (conjunctivalinjection)
● Watery discharge
● Gritty or foreign body sensation
● Photophobia
● Lid swelling
● Blurred vision (if cornea is involved)
● Often starts in one eye, spreads to the other within a few days
73.
Signs
● Conjunctival hyperemia
●Chemosis (conjunctival swelling)
● Follicular conjunctivitis
● Preauricular lymphadenopathy (tender lymph node in front of
the ear)
● Pseudomembrane formation
● Subepithelial infiltrates in the cornea (after 7–10 days)
74.
Diagnosis
● Usually clinical
●Laboratory confirmation:
○ Adenovirus antigen detection via immunoassay
○ PCR for viral DNA
○ Conjunctival swab and culture
75.
Complications
● Subepithelial cornealinfiltrates → may cause blurred vision
for weeks or months
● Pseudomembrane scarring
● Secondary bacterial infection
76.
Treatment
No specific antiviraltreatment; supportive care is the mainstay.
a) Supportive Care
● Cold compresses for comfort
● Lubricant eye drops (artificial tears)
● Topical antihistamines or vasoconstrictors for
itching/redness
77.
b) Topical corticosteroids(with caution)
● May be used in severe inflammation or subepithelial
infiltrates
● Only under ophthalmologist supervision
c) Preventive Measures
● Strict hand hygiene
● Avoid sharing towels, cosmetics
● Disinfect instruments in eye clinics
● Isolation of affected individuals if possible
Bacterial Keratitis
Bacterial keratitisis a corneal infection caused by bacteria,
resulting in inflammation, ulceration, and potential loss of vision
if not treated promptly.
It is one of the most common and sight-threatening ocular
emergencies.
80.
Causes of BacterialKeratitis
Bacterial keratitis is most commonly caused by the following
organisms:
1. Gram-positive bacteria
● Staphylococcus aureus
● Staphylococcus epidermidis
● Streptococcus pneumoniae
Lab diagnosis ofbacterial keratitis
1. Sample Collection
● Corneal scrapings are obtained from the base and edges of
the ulcer using:
○ Sterile spatula or blade
○ Under aseptic conditions, often with topical anesthesia
● Multiple scrapings are taken for:
○ Direct microscopy
○ Culture
89.
2. Direct Microscopy
a)Gram Stain
● Detects Gram-positive or Gram-negative bacteria
● Helps guide initial antibiotic choice
● Shows bacteria and polymorphonuclear leukocytes (PMNs)
b) Giemsa Stain
● Helps visualize inflammatory cells and intracellular organisms
c) KOH wet mount
● Mainly to rule out fungal elements if fungal keratitis is
suspected
90.
3. Culture andSensitivity
● Culture media used:
○ Blood agar (for most bacteria)
○ Chocolate agar (for Haemophilus, Neisseria)
MacConkey agar (for Gram-negative bacilli)
○ Thioglycolate broth (for enrichment)
● Plates are incubated at 35–37°C for 24–48 hours
● Antibiotic sensitivity testing is done using:
○ Kirby-Bauer disk diffusion method
91.
4. Additional Tests
●PCR (Polymerase Chain Reaction) – for rapid and specific
bacterial DNA detection (used in advanced settings)
● Confocal microscopy
Etiology
Primary infection: Oftenasymptomatic or presents as mild conjunctivitis.
Reactivation: Virus remains latent in the trigeminal ganglion and can
reactivate due to:
● Stress
● Fever
● UV exposure
● Trauma
● Immunosuppression
95.
Types
Epithelial Keratitis (mostcommon)
● Site: Corneal epithelium
● Features:
○ Dendritic ulcers (branching pattern with terminal bulbs)
○ Stains with fluorescein and rose bengal
● Symptoms: Pain, photophobia, tearing, foreign body sensation
96.
Stromal Keratitis (Disciformkeratitis)
● Site: Corneal stroma (immune-mediated)
● Features:
○ Stromal edema, central disc-shaped opacity, Descemet’s
folds
○ No active viral replication
● Risk: Scarring and vision loss
Healing of aCorneal Ulcer
A corneal ulcer is an open epithelial defect of the cornea
associated with stromal inflammation, typically due to infection
(bacterial, fungal, viral, or parasitic).
107.
Phases of Healing
1.Initial inflammatory phase
2. Epithelial Regeneration
3. Stromal Repair
4. Endothelial Response
5. Remodeling and Maturation
6. Vascularization (in severe/prolonged ulcers)
108.
1.Inflammatory phase:
First fewhours to 1–2 days
● Events:
- Upon injury or infection, epithelial cells at the ulcer site are lost.
- Inflammatory cells (neutrophils, macrophages) are recruited to
fight infection and remove dead tissue.
- Tear film becomes rich in inflammatory cytokines
- Blood vessels from the limbus may start to invade the cornea if
damage is deep—this is corneal neovascularization.
109.
2. Epithelial Regeneration
Startswithin 24–48 hours
● Migration and proliferation of adjacent healthy epithelial cells.
● Reepithelialization begins within 24–48 hours if the basement
membrane is intact.
● Growth factors (e.g., EGF, TGF-β) assist in healing.
● Limbal stem cells (at the corneal edge) proliferate to replenish
epithelial layers.
● Mitosis increases in nearby healthy epithelial cells.
● As the infection resolves, inflammatory signals reduce.
110.
3.Stromal Repair
Days toweeks depending on ulcer depth
● Keratocytes in the stroma proliferate and synthesize collagen and
proteoglycans.
● May result in scar formation(leucoma) due to disorganized
collagen.
● In deeper ulcers, tissue remodeling can take several weeks or
months
3.Endothelial Response
● The corneal endothelium does not regenerate.
● Remaining cells enlarge and spread to maintain function.
● Damage here may result in corneal edema.
111.
5.Remodeling and Maturation
Weeksto months
● Gradual reorganization of new collagen and ECM.
● Reduction of blood vessels and inflammation.
● Transparency may be partially or fully restored, depending on the
depth and severity of the ulcer.
● Scarring may persist, affecting visual acuity.
5.Vascularization
● in severe/prolonged ulcers
● neovascularization may occur from the limbus to aid healing.
● Can interfere with corneal transparency.
112.
Sequelae/complications of aCorneal Ulcer
● Corneal Scarring (Leucoma)
● Corneal Thinning / Ectasia
● Neovascularization
● Secondary Glaucoma
● Irregular Astigmatism from scarring
● Anterior Synechiae / Posterior Synechiae: Adhesions to the iris
or lens
● Vision Loss
Past questions:
Long essays:
●Enumerate the viruses causing eye infection. Add a note on herpetic
keratitis(2023)
● Give an account on causative agents, pathogenesis and treatment of Mycotic
keratitis(2022)
● Write anatomy and pathology in degeneration of cornea(2022)
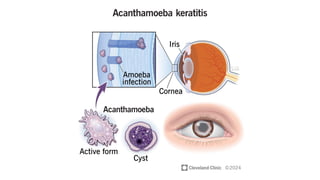
● Write in detail about Acanthamoeba Keratitis(2022, 2015)
● Enumerate the causes of eye infection. Add a note on Herpetic keratitis(2021)
● List the fungal agents encountered in fungal keratitis. Discuss the steps in
laboratory diagnosis of any one of them.(2016)
● Enumerate the viruses causing eye infections. Add a note on herpes simplex
virus(2016)(refer to micro notes for this, not covered adequately in
patho)
● Describe the healing of a corneal ulcer and the sequelae.(2015)
115.
Short essays:
● Acanthamoebakeratitis(2024, 2022, 2023, 2018, 2016)
● Name the causes of bacterial keratitis. Describe the laboratory diagnosis of bacterial
keratitis(2024, 2017)
● Common bacterial infections of cornea and conjunctiva(2023)
● Epidemic keratoconjunctivitis(2022, 2019)
Short answers:
● Name any two Virus causing Eye infections.(2023)
● Name any two fungi causing eye infection(2023, 2022, 2021, 2019)
● What is Acanthamoeba keratitis?(2019)
● Name two bacterial infections of the eye.(2016)
116.
For print-friendly versionof
notes, click here or scan:
References:
- Ramadas Nayak - Textbook of Pathology
for Allied Health Sciences
- A.K Khurana - Comprehensive
Ophthalmology - 7th Ed.
Questions:
salman.s.ansari92@gmail.com
For updated PPT,
click here or scan:












































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















