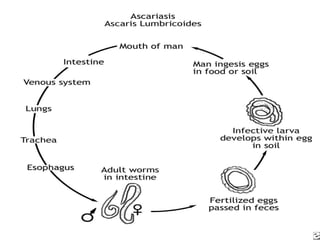
1. Ascariasis is caused by the roundworm Ascaris lumbricoides and is one of the most common helminth infections worldwide, affecting around 1 billion people.
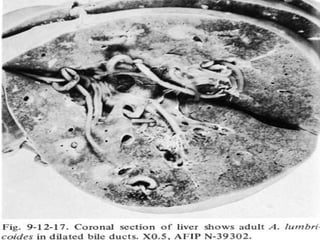
2. Symptoms can include coughing, wheezing and abdominal pain as the worms migrate through the lungs and intestines. Complications can arise if worms cause blockages.
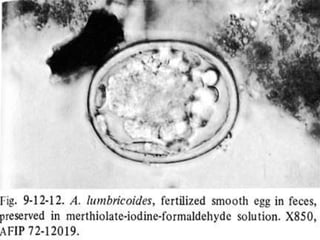
3. Diagnosis is made by examining stool samples under a microscope for Ascaris eggs. Treatment involves oral medications such as albendazole or mebendazole.
























![[Micro] hymenolepis nana](https://cdn.slidesharecdn.com/ss_thumbnails/3rxjz7ekrwinb1sq3uxs-signature-2127a2ca5368c7fdfd023e8d90dde3fc0b9fe7d91346a4189562c9f63dc0d19d-poli-150819190755-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)


























































