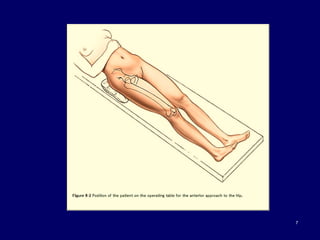
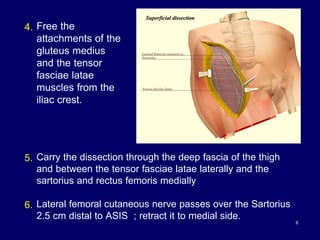
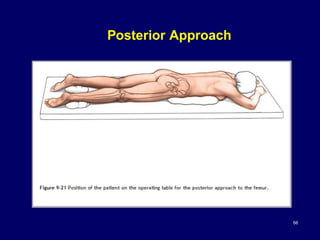
The document describes various surgical approaches to the hip, including anterior, anterolateral, lateral, posterior, and medial approaches. The anterior approach, such as the Smith-Petersen approach, provides access to the front of the hip joint. The lateral approach, including the Hardinge and Watson-Jones approaches, avoids the need for trochanteric osteotomy. The posterior, or Moore's, approach is the most commonly used and provides exposure for procedures like hip replacements. Each approach has specific indications and technical steps described. Potential dangers to nerves and blood vessels are also outlined.