Download to read offline









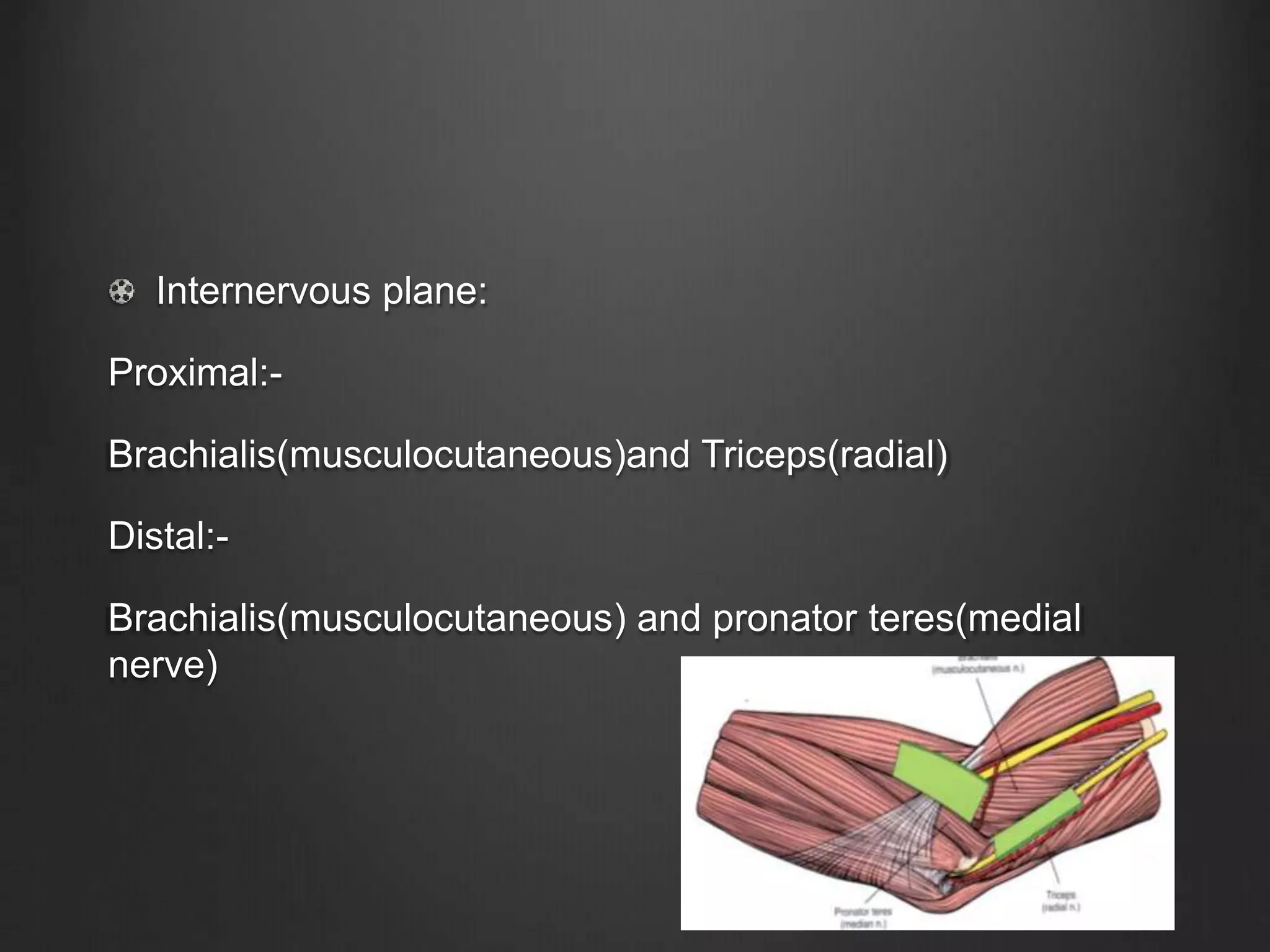










This document describes three cases involving surgical approaches to the elbow. Case 1 describes a postero-lateral approach for a 55-year old female with tenderness over the radial head after a fall. The incision is made directly over the radial head between the anconeus and ECU muscles. Case 2 describes a medial approach for a 39-year old male with decreased elbow range of motion after a fall. The incision is centered over the medial epicondyle between the pronator teres and brachialis muscles. Case 3 describes an antero-lateral approach for an 80-year old male with an elbow deformity and no range of motion after a fall. The inc























































































