Downloaded 508 times

![1.Individual indices
2.Group indices
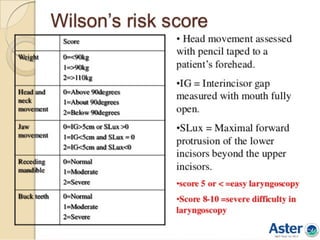
Wilson’s score
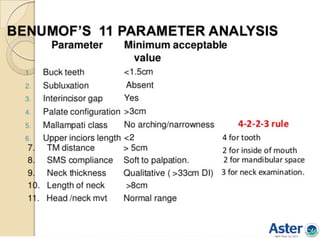
Benumof’s analysis
Saghei & safavi test
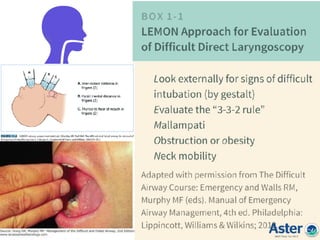
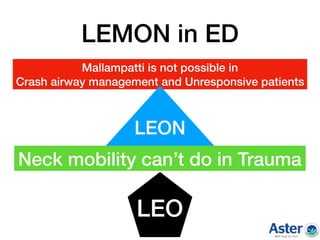
Lemon assesment
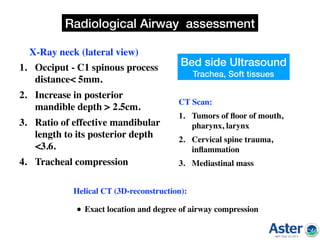
3.Radiological indices
Airway assessment indices
a)X Ray Neck[Lataral]
b)CT Scan
c)Helical CT
d)USG
4.Advanced
indices
• Flow volume
loop
• Acoustic
response
measurement
• Ultra sound
guided
• CT/MRI
• Flexible
bronchoscope](https://image.slidesharecdn.com/airwaypushpagiri-180429065526/85/Difficult-airway-Made-easy-9-320.jpg)











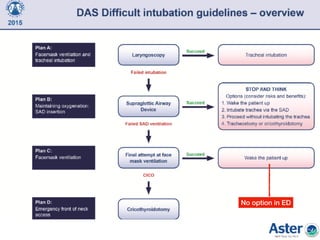




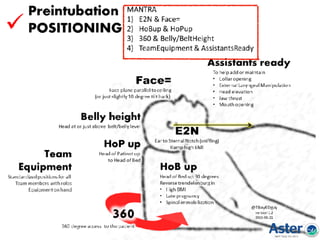


vital role Pre-oxygenation: vital Awake intubation: consider Alternative airway: have ready Senior help: call early Cricothyrotomy: know how to do Postpone if not urgent Don't panic, think and act Document: vitally important Prepare for worst Train and practice regularly























































































