Downloaded 112 times

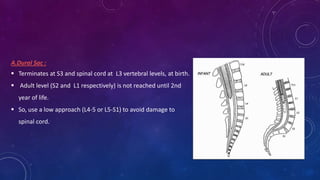
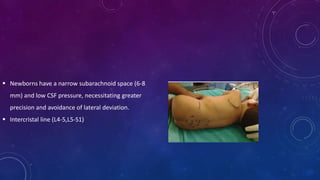
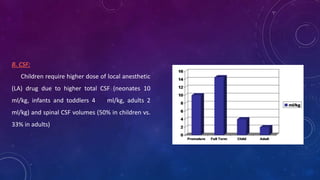


Spinal anesthesia can be used as a primary anesthetic technique in children, especially for former preterm infants to reduce postoperative apnea risk compared to general anesthesia. Key differences in pediatric spinal anatomy and physiology require lower needle insertion points and higher local anesthetic doses in children. Spinal anesthesia provides effective pain control and fewer cardiovascular and respiratory complications than general anesthesia for many pediatric surgeries under 90 minutes. Complications are generally minor when performed carefully according to age-specific anatomical considerations and monitoring.

![The basics of peds anesthesia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/thebasicsofpedsanesthesiaautosaved-111017032903-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)






