Downloaded 160 times





















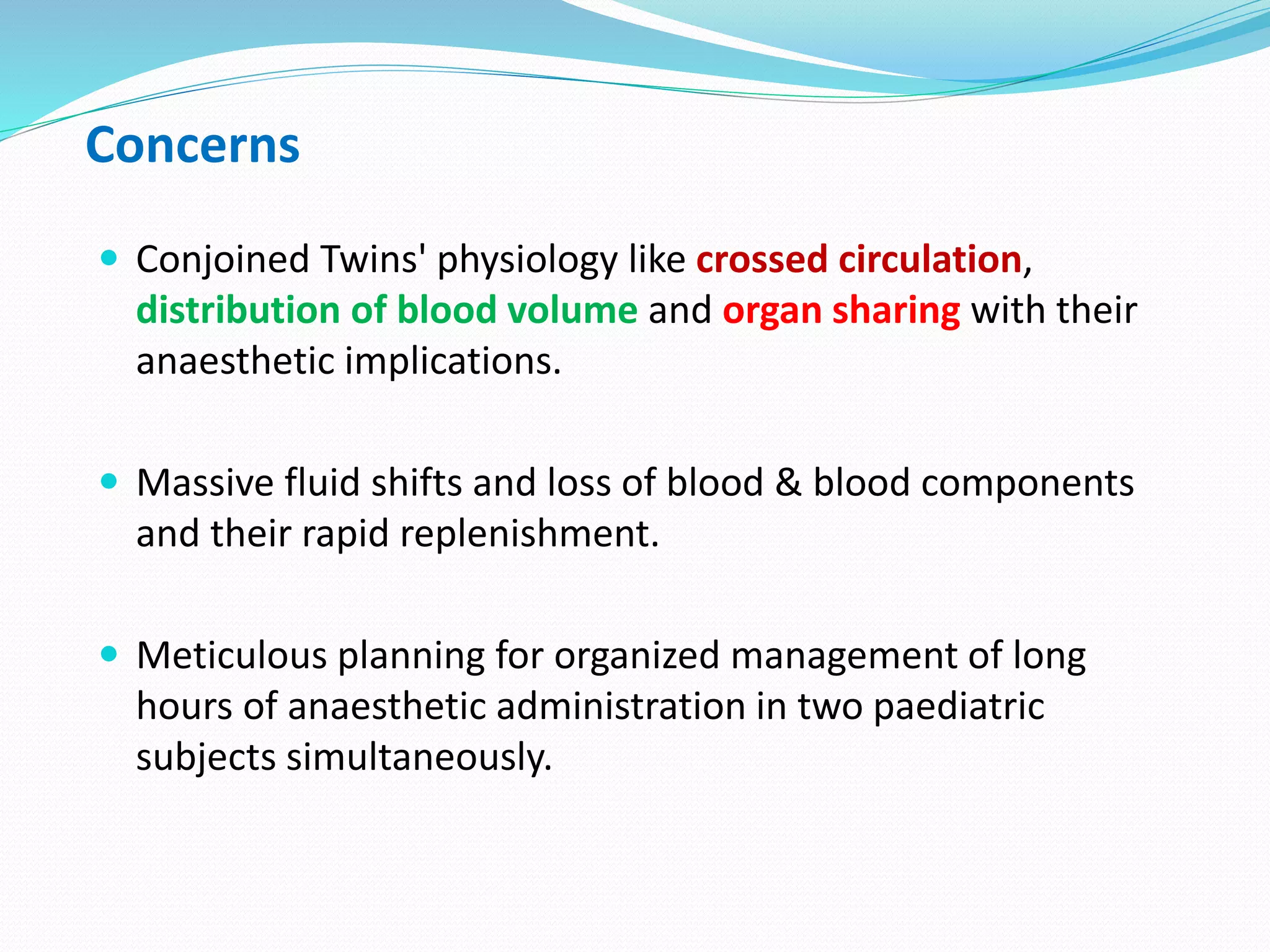

























Dr. Kumar presented on the topic of conjoined twins. Some key points: - Conjoined twins occur in approximately 1 in 50,000 births and are always the same sex. They result from a single fertilized egg that only partially splits. - Classification is based on the point of conjunction. The most common types are thoracopagus (chest) and omphalopagus (abdomen). - Separation surgery requires extensive planning due to risks of circulatory mixing between twins. Careful monitoring and individualized dosing of anesthesia drugs is needed. - The challenges include potential airway issues, assessing cardiovascular and respiratory systems, and ensuring adequate monitoring and equipment for each twin. Metic






























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)