
Downloaded 113 times























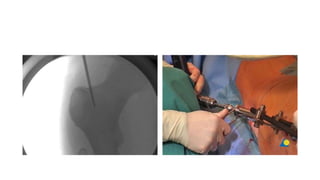





















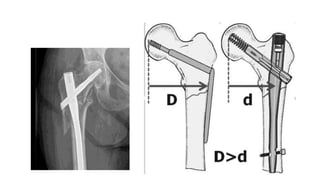




The document discusses classifications and treatment approaches for subtrochanteric fractures of the femur. It describes Fielding and Seinsheimer classifications which categorize fractures based on their location and number of fragments. Temporary options include a Thomas splint for unstable patients. Surgical treatments involve plates, intramedullary nails, or external fixators. Precise surgical approaches depend on the fracture location and stability. Potential complications are also noted.























































































