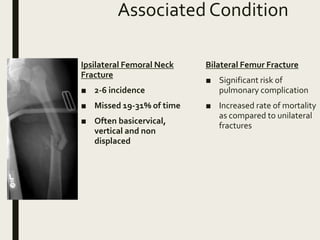
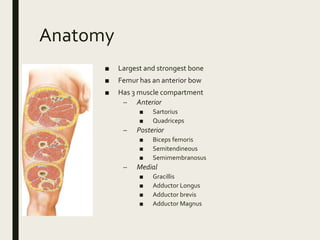
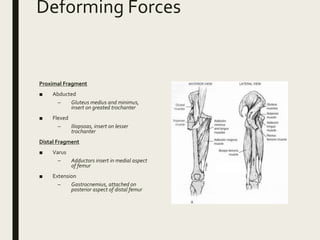
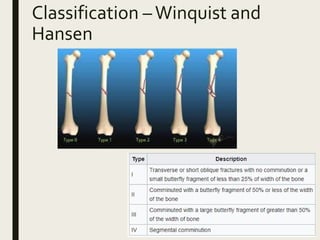
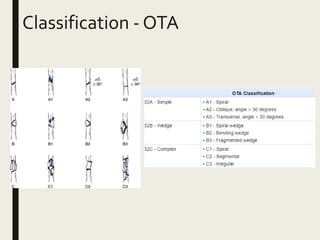
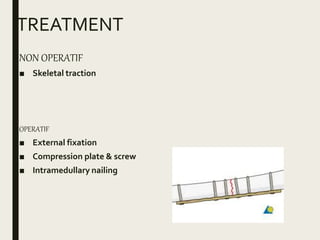
This document discusses fractures of the femur shaft. It begins by noting that femur fractures are often associated with high-energy injuries and have an incidence rate of 37.1 per 100,000 people per year. Younger patients typically experience fractures from falls or motor vehicle accidents while older patients' fractures are often due to osteoporosis or neoplasms. Associated injuries include ipsilateral femoral neck fractures which are missed 19-31% of the time. Treatment involves restoring alignment, length, stability and range of motion through non-operative or operative means such as intramedullary nailing or plating. Post-operative care focuses on early range of motion exercises while delaying weight bearing and strengthening.



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








