Download as PDF, PPTX












![Explanation to Alcohol and Sexual Dysfunction
From Virginia Alcohol Safety Action
Program ([VASAP], 2002), alcohol interferes
with the normal production and
maintenance of female and male
hormones.
For women, this can mean changes in the
menstrual cycles and a decreased or loss of
ability to be become pregnant.
19-Mar-16 asareor@yahoo.com 2016 46](https://image.slidesharecdn.com/substancerelateddisorders-alcoholism-181218030322/75/Substance-related-disorders-alcoholism-46-2048.jpg)




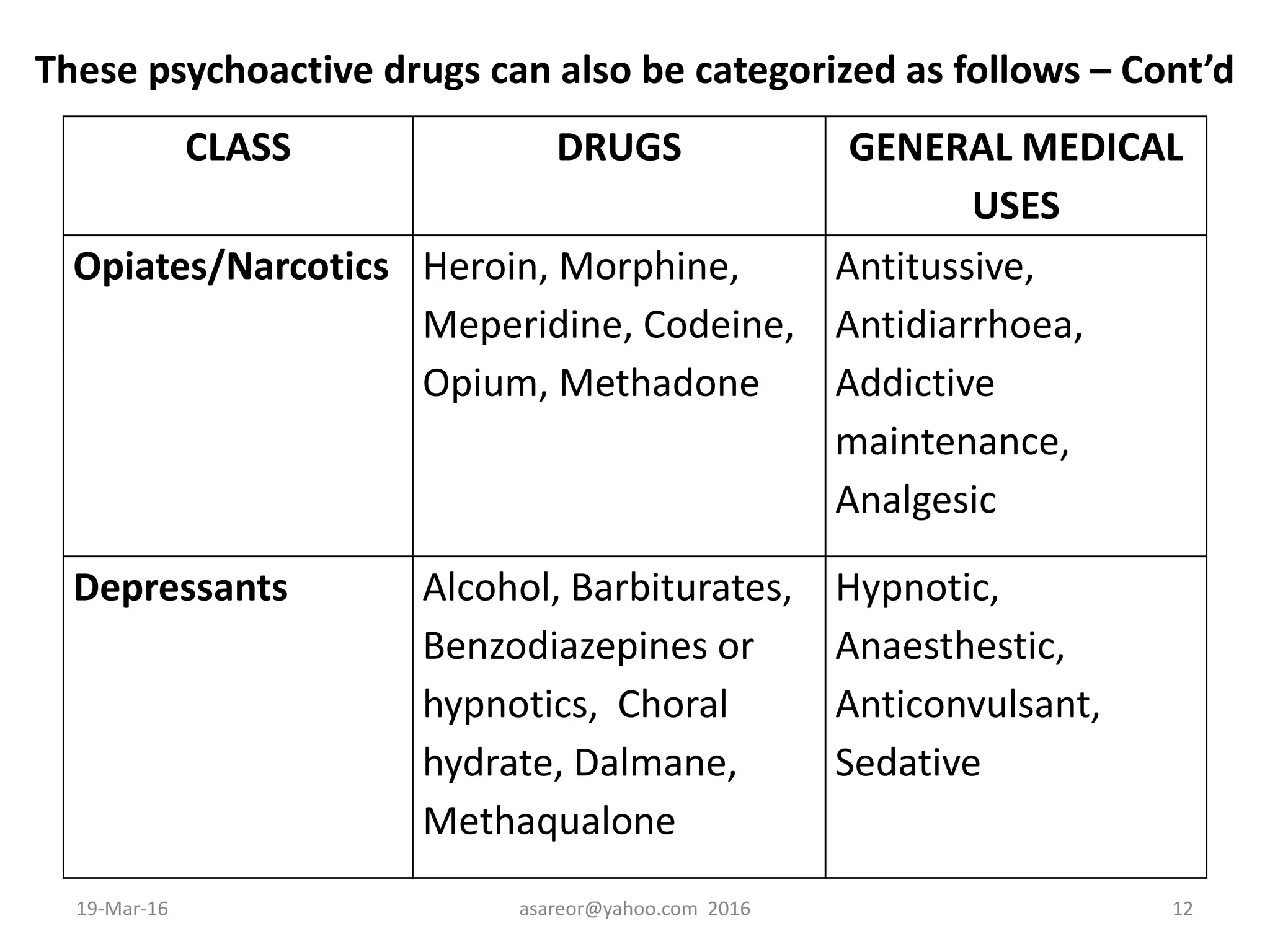
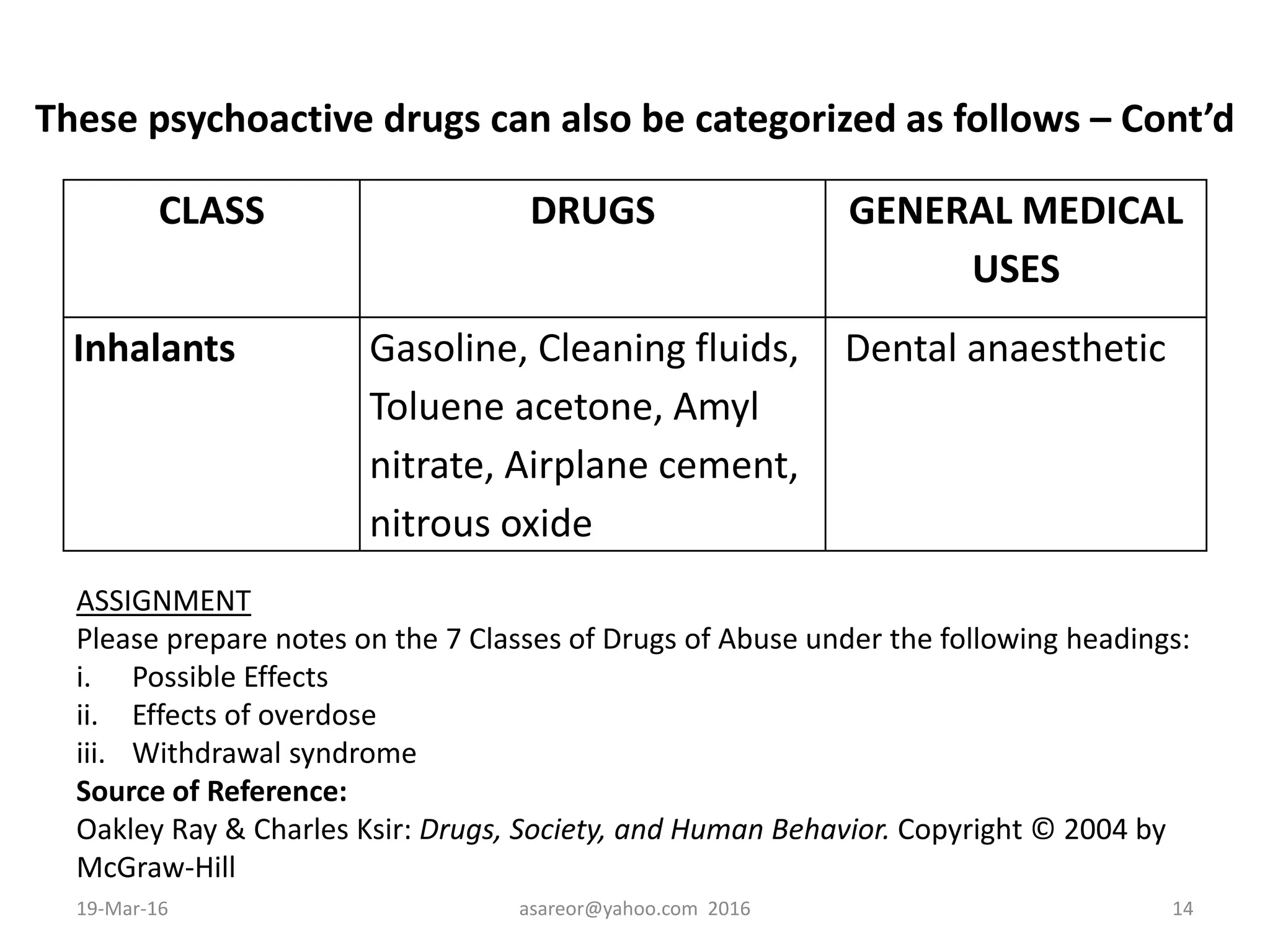
The document discusses substance related disorders and alcoholism. It defines key terms related to substance use and dependence. It also categorizes psychoactive drugs and lists their medical uses. The document discusses causes of substance disorders including biological, psychological, and sociocultural factors. It provides signs of drug addiction and key nursing interventions for substance abuse treatment. Finally, it defines alcoholism and provides medical definitions of the disorder.




































































![Rheumatic Fever CASE PRESENTATION [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationautosaved-251123182512-9d9b0da4-thumbnail.jpg?width=640&height=640&fit=bounds)

















