Download as PDF, PPTX

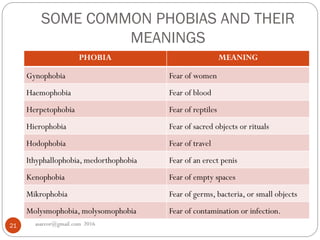
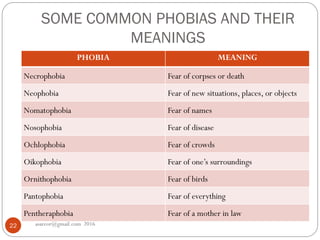
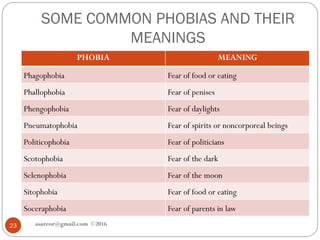
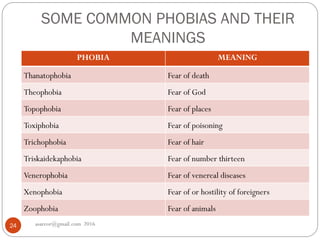


This document provides an overview of anxiety disorders, including definitions of anxiety, differences between normal and pathological anxiety, and descriptions of specific anxiety disorders. It discusses phobias as a type of anxiety disorder characterized by irrational and intense fears of specific objects or situations. The document outlines several common phobias like agoraphobia, social phobia, and specific phobias, and provides examples of specific phobias like fears of heights, animals, and social interactions.











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










