Downloaded 1,105 times



































































![• The effectiveness of yoga in treating PTSD is unclear.
Two RCTs found opposite effects in two dissimilar
patient populations, while one systematic review
concluded that yoga may be effective as a
monotherapy or in combination with medication for
treating patients with PTSD.
• The effectiveness of mindfulness in treating PTSD is
unclear. Three RCTs found opposite effects in
veterans with PTSD.
Yoga for the Treatment of Post-Traumatic Stress Disorder, Generalized Anxiety Disorder, Depression, and Substance
Abuse: A Review of the Clinical Effectiveness and Guidelines [Internet]. Ottawa (ON): Canadian Agency for Drugs and
Technologies in Health; 2015 Jun.
Mindfulness Interventions for the Treatment of Post-Traumatic Stress Disorder, Generalized Anxiety Disorder,
Depression, and Substance Use Disorders: A Review of the Clinical Effectiveness and Guidelines [Internet].
Source
Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2015 Jun.](https://image.slidesharecdn.com/posttraumaticstressdisorder-151027125212-lva1-app6891/75/Post-traumatic-stress-disorder-84-2048.jpg)




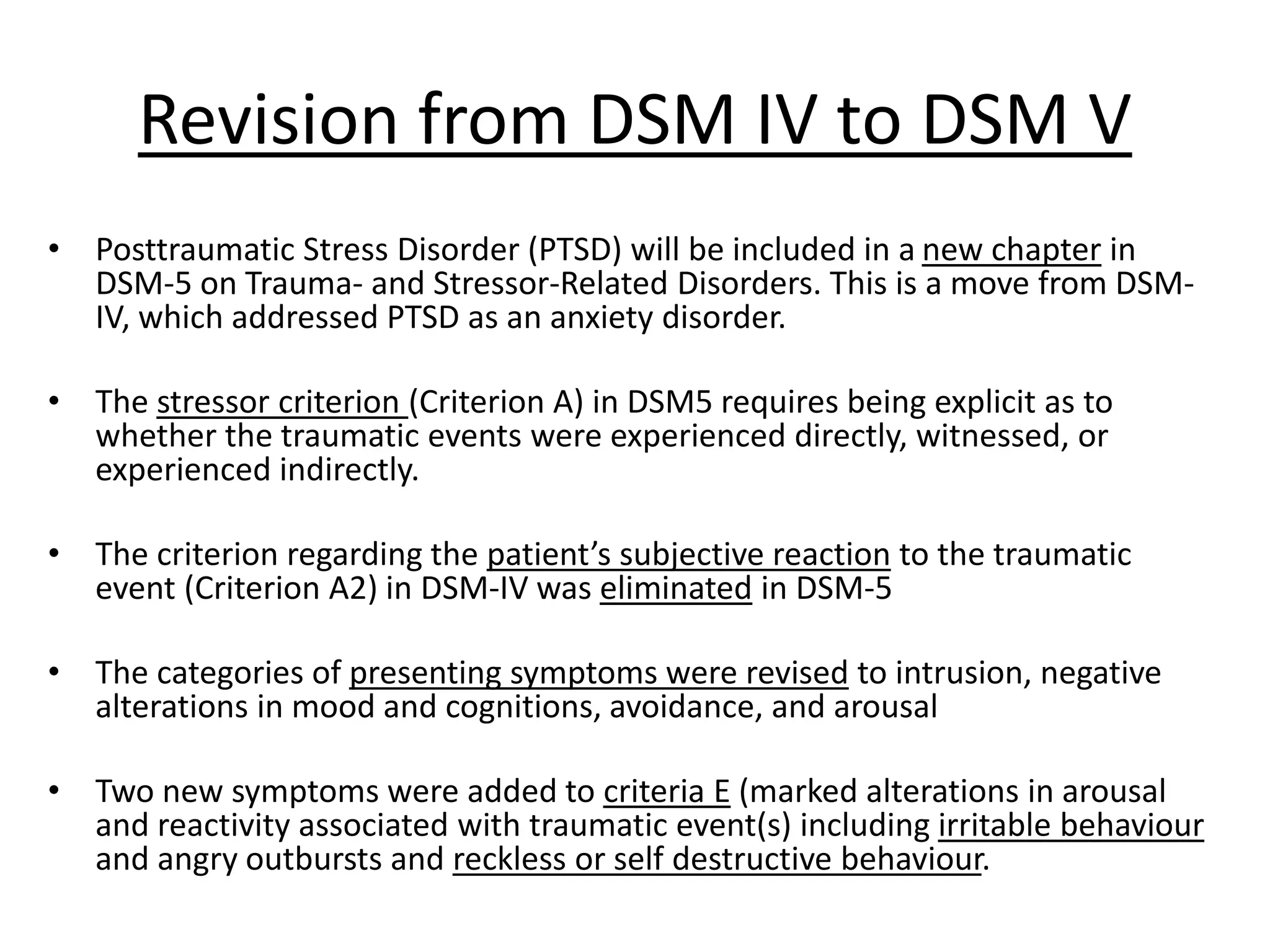
The document discusses post-traumatic stress disorder (PTSD), covering its historical context, definition, epidemiology, risk factors, and treatment options. PTSD is characterized by symptoms such as intrusive memories, avoidance behavior, and heightened arousal, often following traumatic events like combat, assault, or disaster. It highlights the prevalence of PTSD, particularly among different demographics, and stresses the importance of diagnosis and management strategies in clinical settings.






































![Original aapb alba presentation 2-97-2003-march [autosaved] (2 - copy](https://cdn.slidesharecdn.com/ss_thumbnails/originalaapbalbapresentation-2-97-2003-marchautosaved2-copy-160721070506-thumbnail.jpg?width=640&height=640&fit=bounds)




























