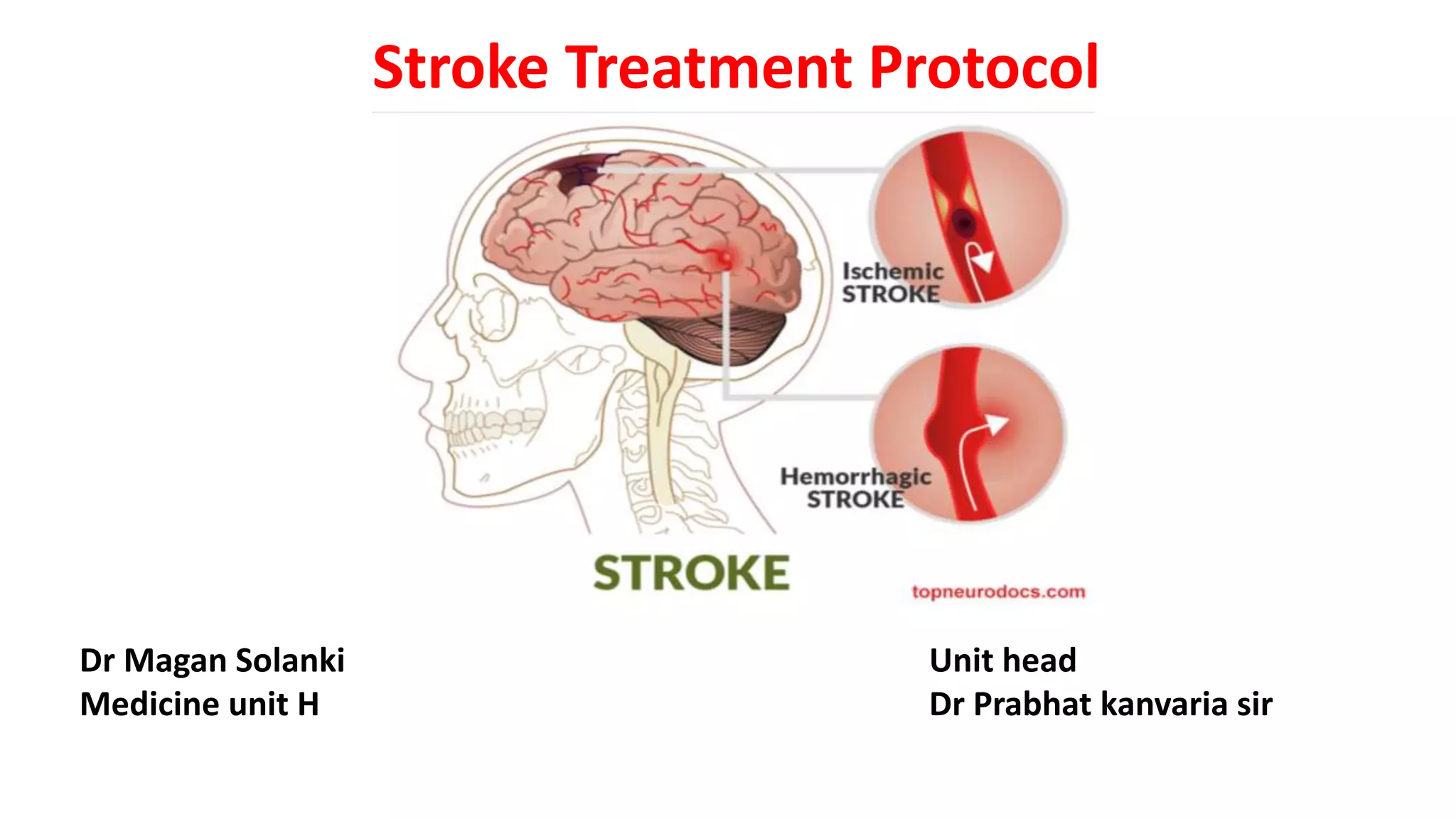
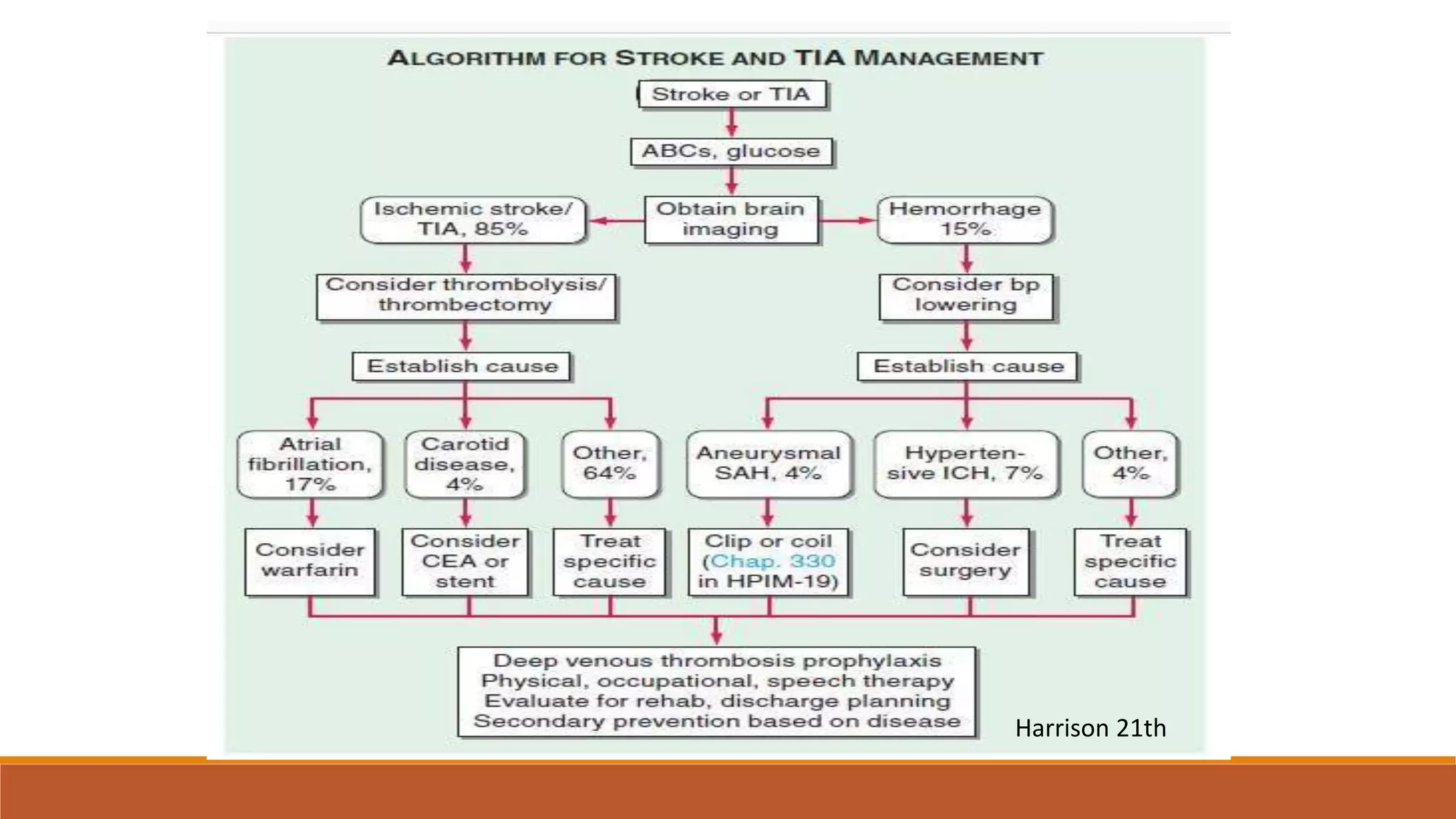
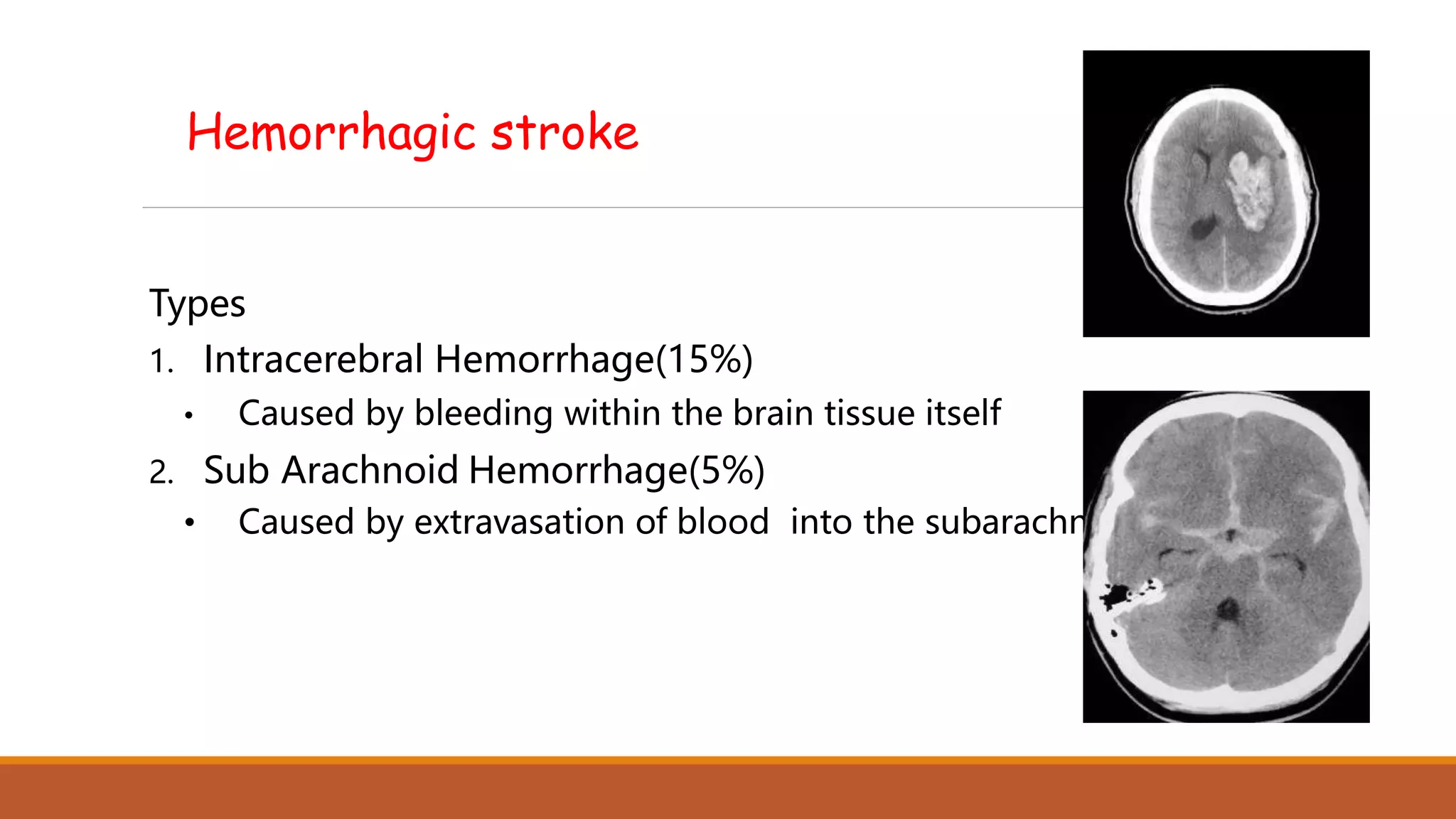
1. Stroke can be caused by blockage of blood flow (ischemic) or bleeding in the brain (hemorrhagic). Treatment depends on the type and location of stroke.
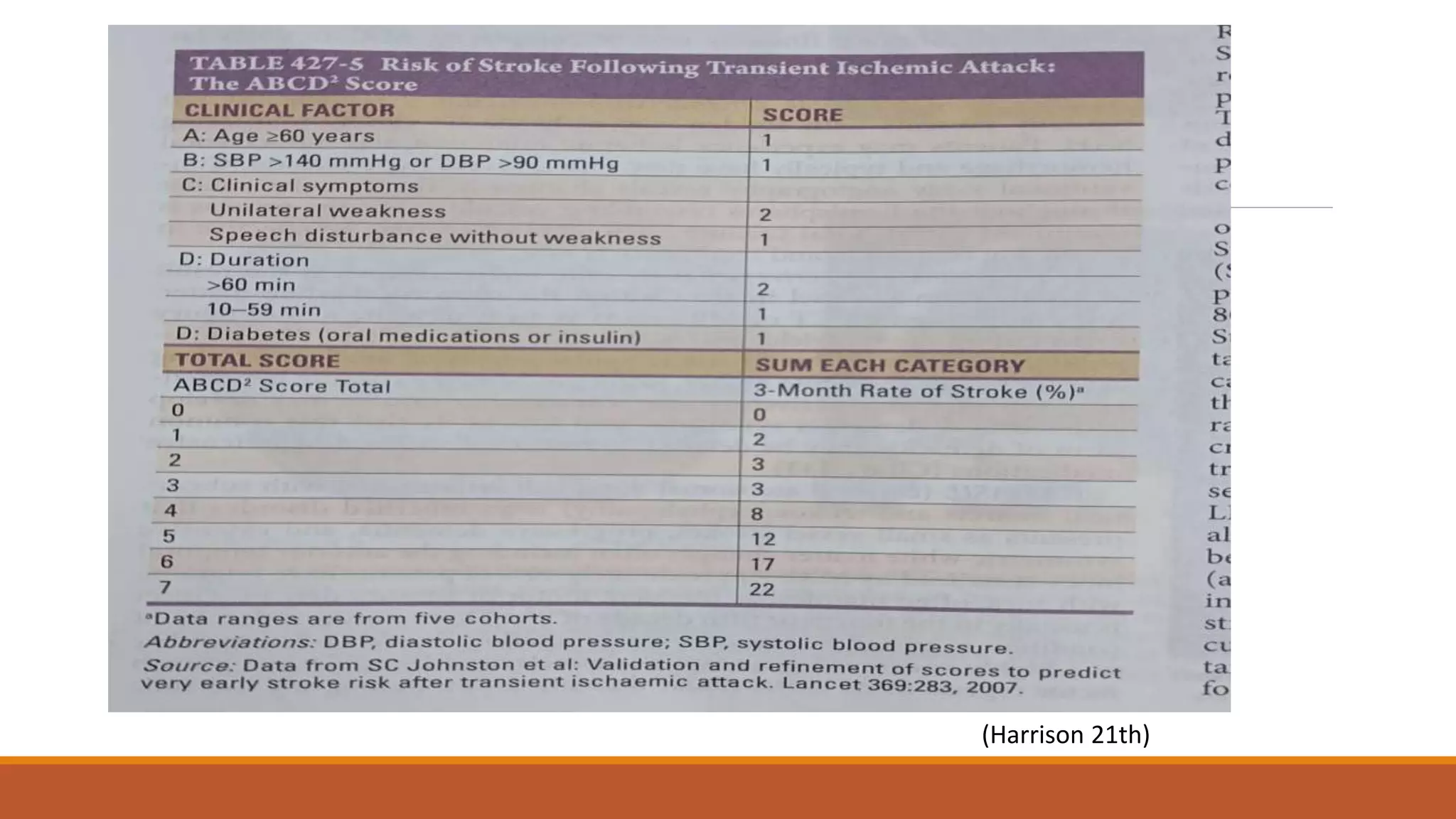
2. Risk factors for stroke can be modifiable like hypertension, diabetes, smoking or non-modifiable like age, sex, family history. Managing modifiable risk factors is important for prevention.
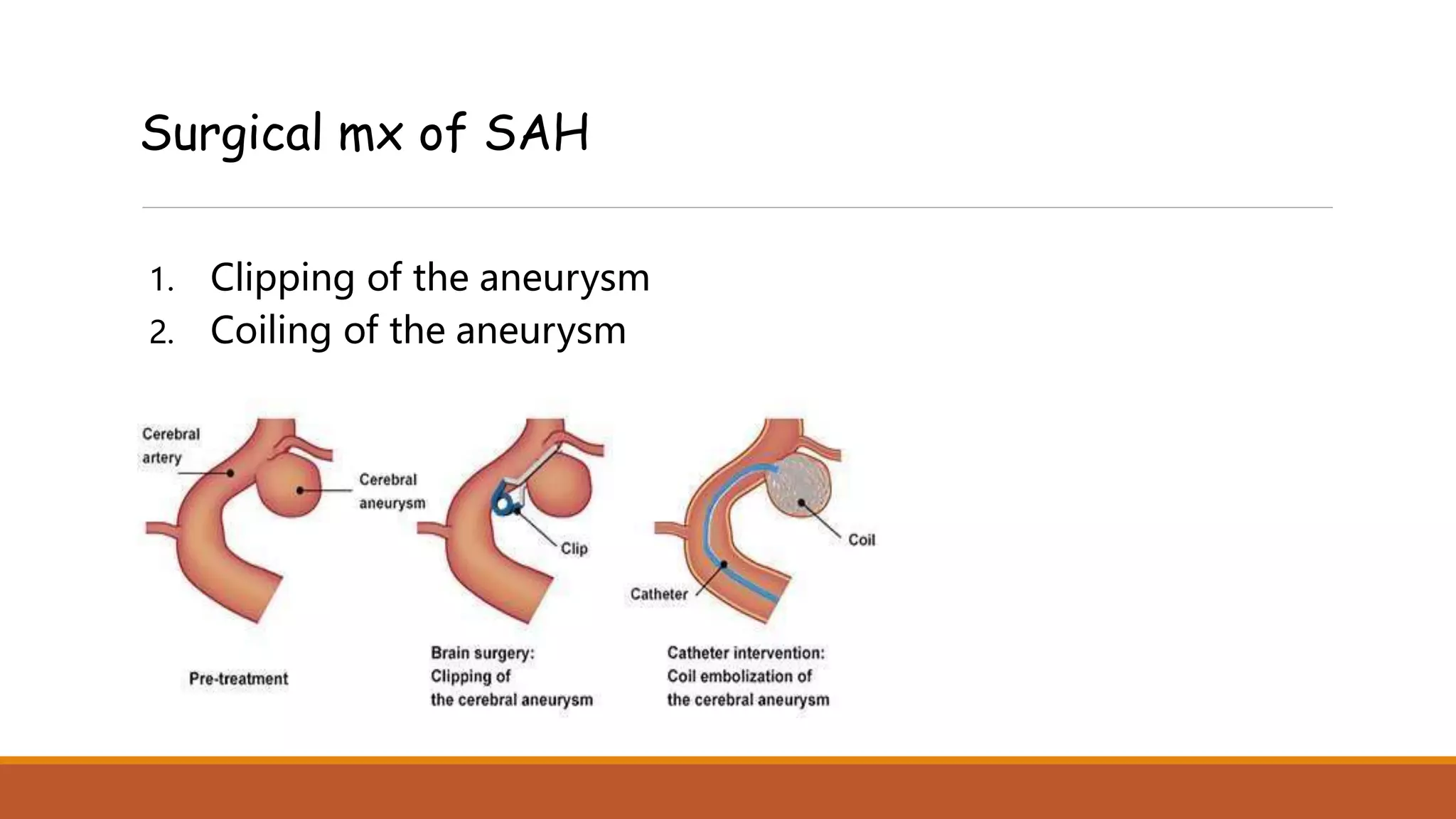
3. Acute treatment of ischemic stroke may involve clot-busting drugs intravenously or surgery to remove clots, while hemorrhagic stroke management focuses on controlling blood pressure, reducing swelling in the brain.







![[NCCT]
{NCCT}
C](https://image.slidesharecdn.com/stroketreatmentprotocol-230117191606-5d10ddee/75/Stroke-Treatment-Protocol-pptx-12-2048.jpg)















![Management- ICH
1. Blood Pressure- <140 [sbp]
IV medications
• Labetalol
• Nicardipine
• Esmolol
• Enalapril
• Hydralazine
• Nitroglycerine](https://image.slidesharecdn.com/stroketreatmentprotocol-230117191606-5d10ddee/75/Stroke-Treatment-Protocol-pptx-29-2048.jpg)