Downloaded 35 times


![MEDICAL DIAGNOSIS OF STROKE
History and examination
Tests and measures
Use of NIHSS National Institutes of Health Stroke Scale
Blood analysis
Imaging .. CT scan, MRI
Pharmacologic Management or surgical management…
Thrombolytics tPA.. Tissue plasminogen activator
Anticoagulants (e.g., warfarin [Coumadin], heparin, dabigatran
etexilate [Pradaxa])
Antiplatelet therapy (e.g., acetylsalicylic acid [aspirin]; clopidogrel
bisulfate [Plavix]; dabigatran etexilate [Pradaxa]; ticlopidine
hydrochloride [Ticlid])
Antihypertensive agents (e.g., ACE inhibitors, alpha-blockers
[Minipress], beta-blockers, calcium channel blockers, direct
vasodilators, diuretics, postganglionic neuron inhibitors
Angiotensin II receptor antagonists (telmisartan [Micardis], losartan
potassium [Cozaar])
Antispastics, anticonvulsants, antidepressants.](https://image.slidesharecdn.com/stroke-170702184553/85/Stroke-43-320.jpg)


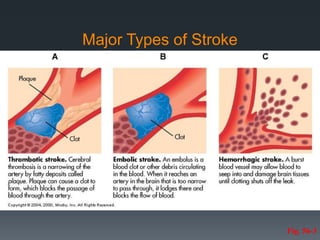
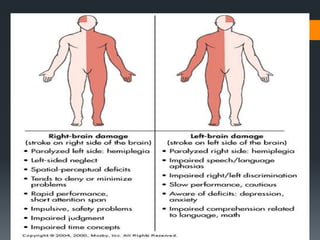
The document discusses stroke, including its pathophysiology, types, risk factors, and management categories. Key points include: - Stroke is caused by interrupted blood flow to the brain and can be ischemic (caused by clots or blockages) or hemorrhagic (caused by bleeding). - Major risk factors include age, gender, race, family history, diabetes, heart disease, smoking, hypertension, and obesity. - Strokes are classified based on location and cause, such as thrombotic, embolic, or hemorrhagic strokes. - Complications include sensory and motor deficits, speech/swallowing issues, and cognitive/emotional changes.
































![Stroke [uncensored] - by MHR Corporation](https://cdn.slidesharecdn.com/ss_thumbnails/mhr4-stroke-101129110104-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































