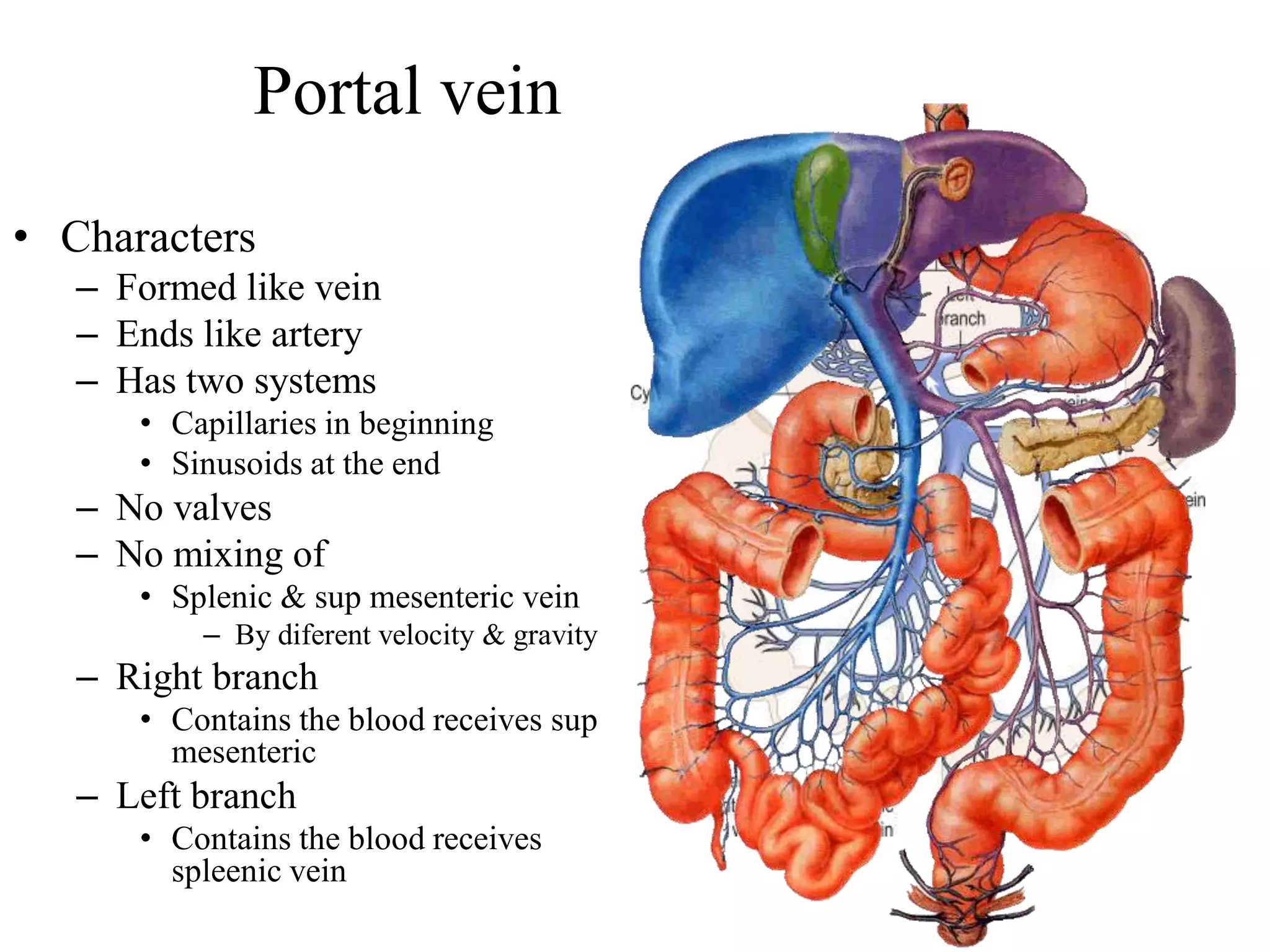
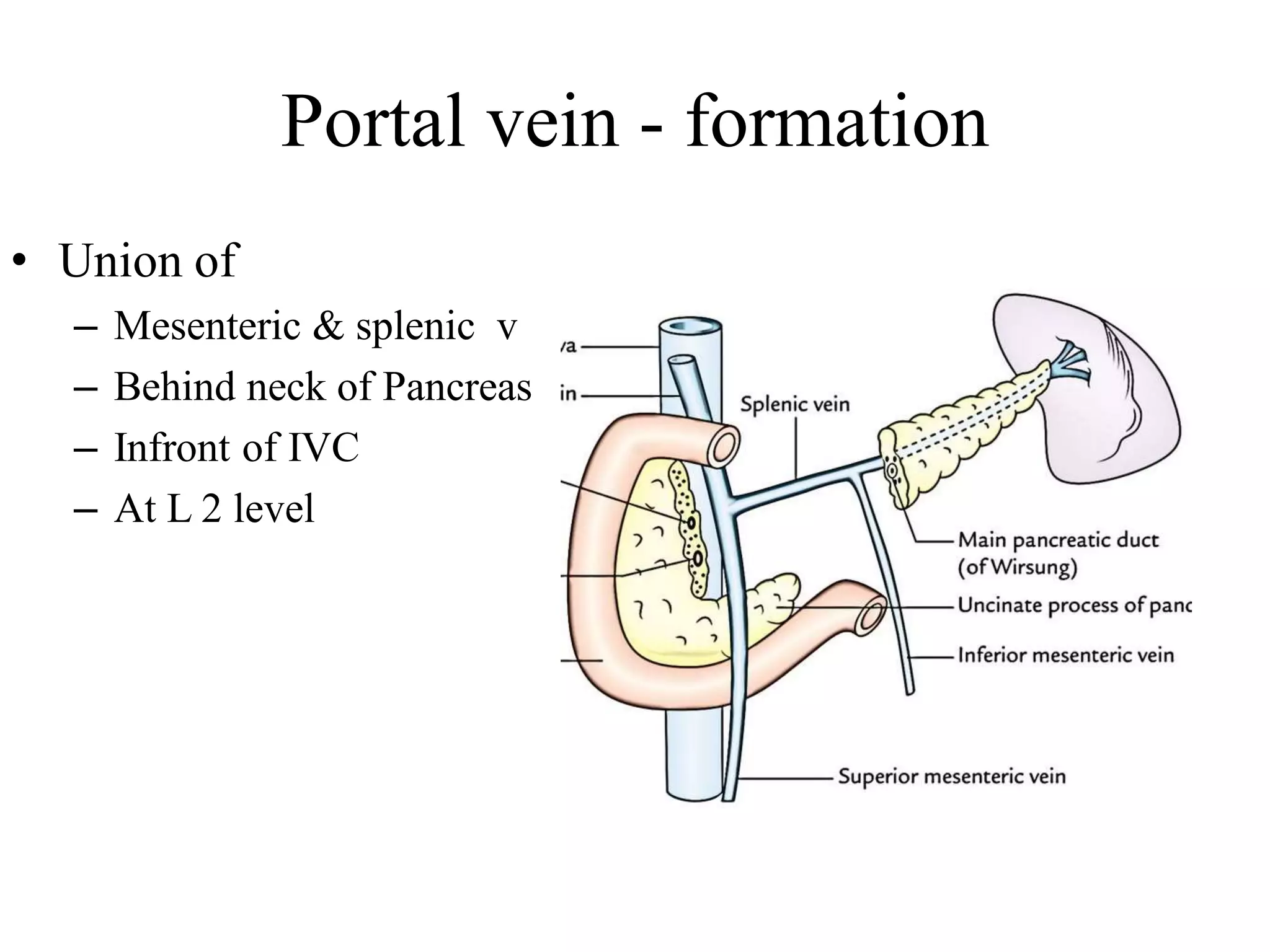
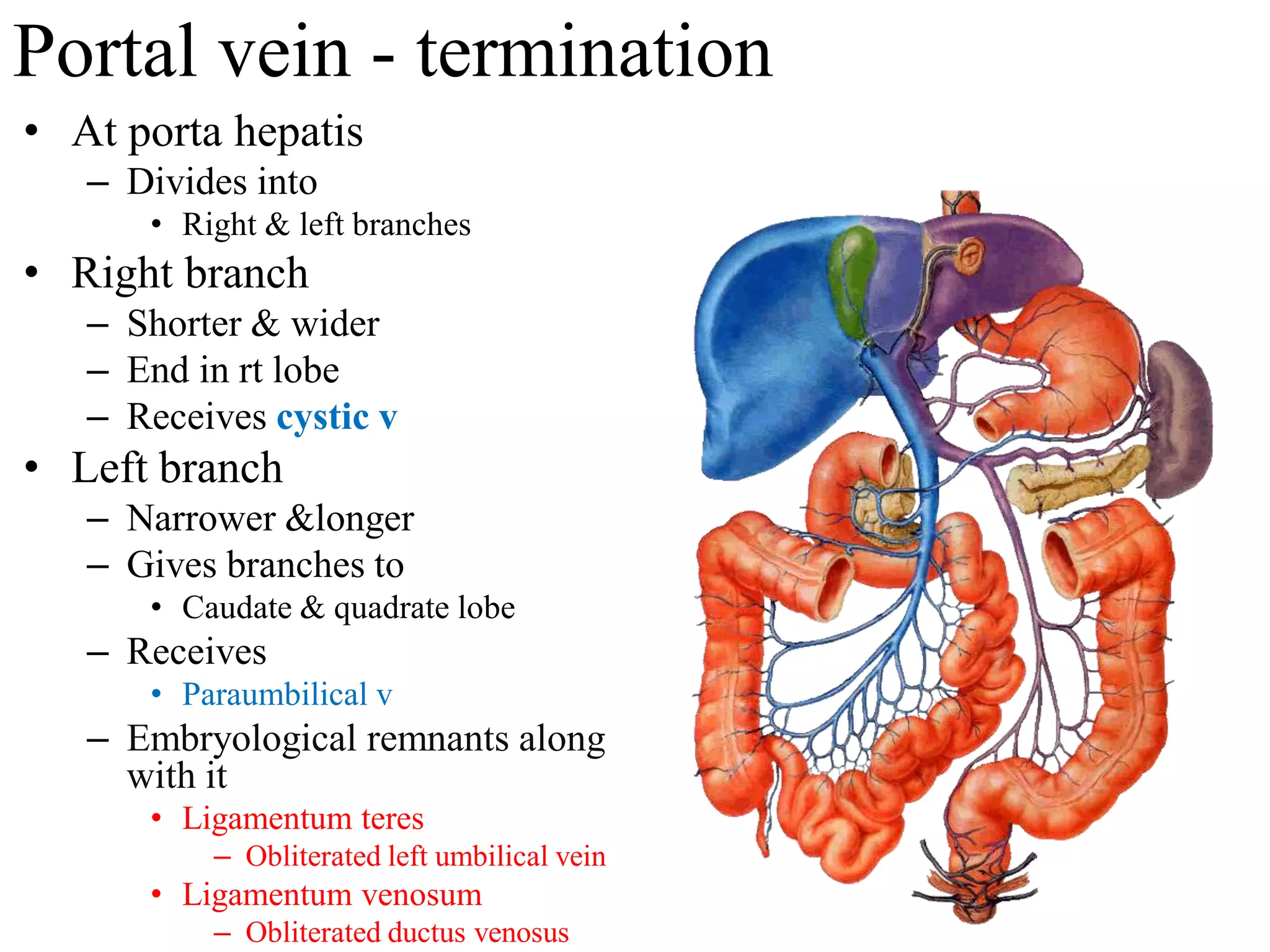
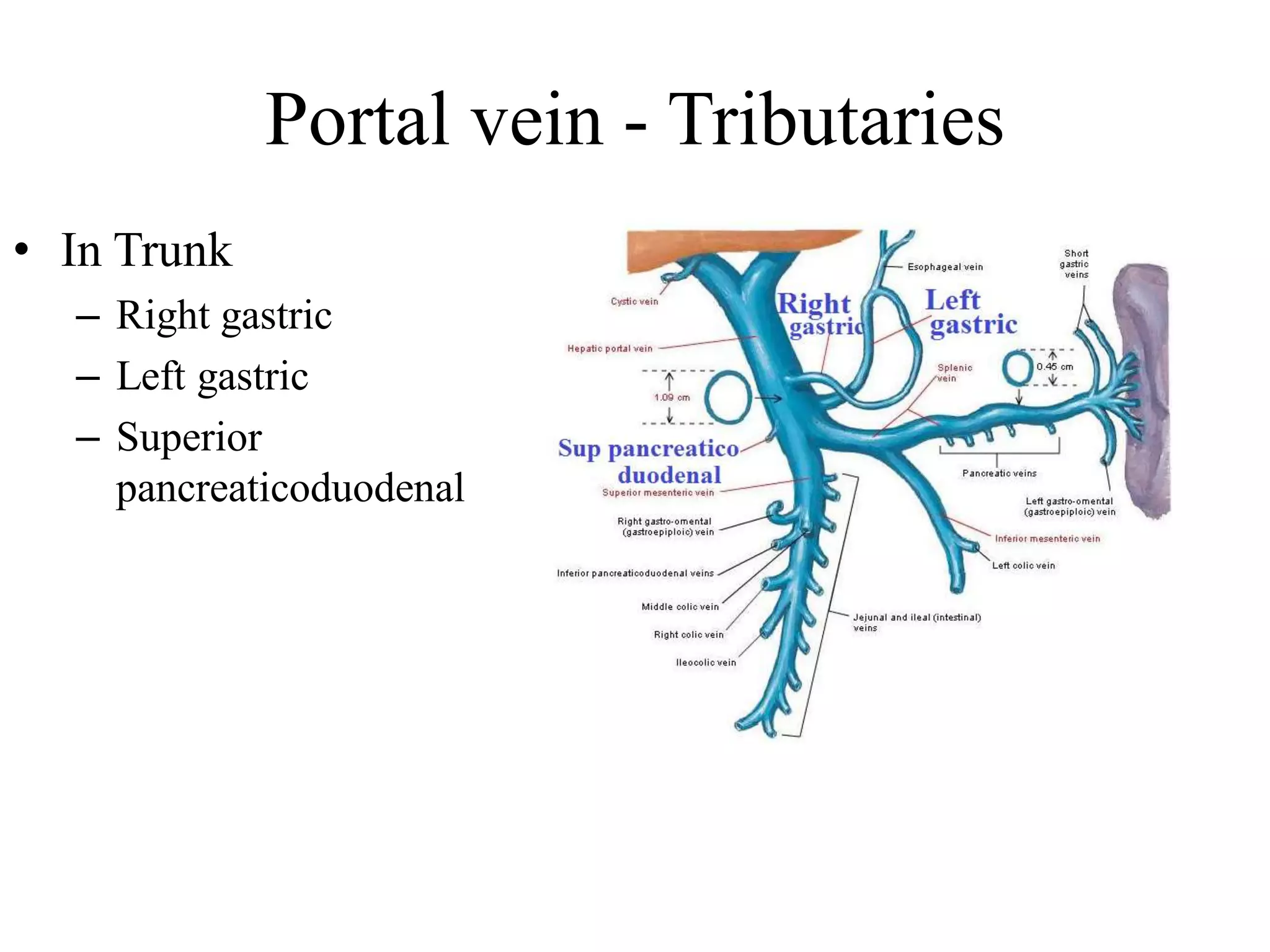
This document describes the anatomy and vasculature of the spleen and portal vein. It notes that the spleen is located in the left hypochondrium between the stomach and diaphragm. The portal vein collects blood from the gastrointestinal tract and transports it to the liver. When the portal vein is obstructed, as in cirrhosis, portal hypertension can develop leading to splenomegaly and collateral circulation through portosystemic anastomoses.