PORTAL
CIRCULATION
Blood is collectedfrom one set of capillaries and
is passed to a larger vessel which then again
divides into capillaries before the blood is
returned to systemic circulation.
4.
Portal vein
Origin &end in capillaries / venous
sinusoids
• Size: 8cm X 1 cm
• Drains
– Abdominal part of alimentary
tract (except lower part of anal
canal)
– Spleen ,Pancreas,gallbladder,
• Conveys absorbed products of
digested food to liver
• Devoid of valves
• Reservoir of blood : 1200 ml /
min
5.
Features
1. It providesabout 80% of the blood that flows through
liver.
2. Its tributaries and branches contain up to one-third of
the total volume of blood in the entire body.
3. The portal vein and its tributaries are devoid of valves.
4. It transports the products of digestion of carbohydrates,
proteins, and other nutrients from the intestine and also
products of red cell destruction (etc.) from the spleen to liver.
5. It divides into branches which, like those of hepatic
artery, discharge their blood into sinusoids of the liver,
which are drained by hepatic veins into the IVC.
6. It begins like vein from capillary bed of the gut and
terminates like an artery in the hepatic sinusoids.
6.
Formation
– Union ofSup
mesenteric & Splenic
vein
– Between neck of
Pancreas & IVC at
level L2
7.
Course: Extrahepatic part
•Passesupwards & Rt, behind neck of pancreas & 1st part
of duodenum
• Enters rt free margin of lesser omentum in front of
epiploic foramen with BD & HA
• Reaches porta hepatis & divides into rt & Lt branches.
8.
Course: Intrahepatic part
•Branches of portal vein
• – Segmental brs
• – Brs in Portal canal
• – Hepatic sinusoids
• – Central veins
• – Sublobular veins
• – Hepatic veins
• IVC
9.
Branches
• Formative
– SupMesenteric vein
– Splenic vein
• Received by Trunk
– Rt & lt Gastric veins
– Superior PD vein
• Received by branches
– Cystic vein
– Paraumbilical veins
• Occasional
– Inf mesenteric
– Rt gastro-epiploic
– Pre-pyloric vein
Rt Branch
Shorter, wider, Receives cystic vein
Lt branch
Narrower, longer, Runs in Porta hepatisnfrom Rt to Lt
Brs to Caudate & Quadrate lobe
Receives Paraumbilical veins
15.
Parts
• Infraduodenal
liesbelow the first part of
duodenum.
• Retroduodenal
lies posterior to first part of
duodenum
• Supraduodenal
lies above the first part of
duodenum in right free margin
of lesser omentum
16.
Relations
Infra duodenal
– Ant:Neck of Pancreas
– Post: IVC
Retro duodenal
– Ant: Duodenum (1st Part),
Bile duct, GD artery
– Post: IVC
Supra duodenal : In rt free
margin of lesser omentum
– Ant : hepatic artery & bile
duct
– Post: IVC
• Surrounded by Hepatic plexus
of nerves, lymphatics & LN
17.
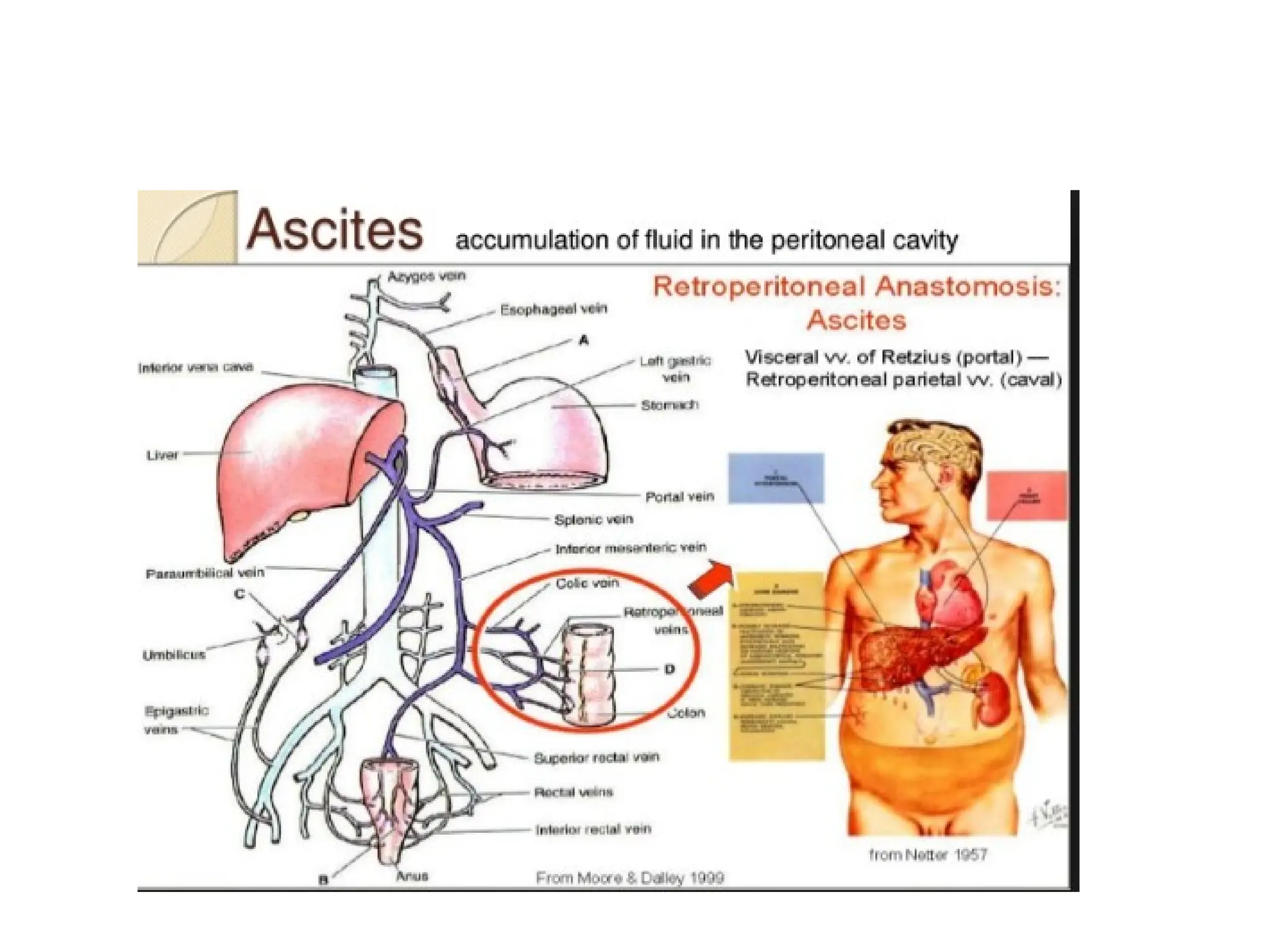
Portocaval anastomosis
Sites inabdominal cavity
where anastomosis exists
between the portal and
systemic venous
systems.
These communications
between the veins of the
portal and caval (systemic)
systems form important
routes of collateral
circulation in cases of
portal obstruction.
18.
Portocaval anastomosis
1. Umbilicus:Here left branch of portal vein
communicates with superficial veins of
anterior abdominal wall around umbilicus,
through paraumbilical veins (of Sappey).
19.
2.Lower end ofesophagus: Here esophageal tributaries
of left gastric vein (draining into portal vein)
anastomose with esophageal tributaries of accessory
hemiazygos vein (systemic).
20.
3. Anal canal:Here superior rectal (hemorrhoidal) vein
which ultimately drains into portal vein anastomoses
with middle and inferior rectal veins, tributaries of
internal iliac (systemic) vein.
21.
4. Extraperitoneal surfacesof retroperitoneal organs:
Veins of retroperitoneal organs such as duodenum,
ascending colon, and descending colon (portal)
anastomose withretroperitoneal veins of
posterior abdominal wall and renal capsule (systemic).
The renal vein anastomosis with splenic and azygos
veins.
22.
5. Bare areaof liver: Here the hepatic venules
(portal) anastomose with phrenic and
intercostal (systemic) veins.
Portal hypertension
• Obstructionof the portal vein or its branches
leads to increase in portal venous pressure
called portal hypertension, i.e., pressure above
40 mmHg (normal being 5–15 mmHg). This
leads to enlargement of collateral channels.
> 12 mm of Hg
• Causes :
– Pre hepatic : Thrombosis of portal vein
– Hepatic: Cirrhosis
– Post hepatic: Budd-Chiari Syndrome
Esophageal varices
• Inportal obstruction as in liver cirrhosis, these
collateral channels become distended and
tortuous, forming esophageal varices, which
may rupture causing hematemesis (vomiting of
blood) and may even bleed to death.
29.
Caput Medusae
In portalobstruction, the superficial veins around the
umbilicus become distended and tortuous (varicosity).
This whorl of prominent distended tortuous (snake-like)
veins aroundn the umbilicus is known as caput medusae1
—a sign of diagnostic value to the clinicians.
30.
Hemorrhoids
• The distension
anddilatation of
these
anastomotic
channels result in
the formation of
hemorrhoids or
piles which may
be responsible for
repeated bleeding
per annum