Here are some key questions this summary could address:
- What are some common uses and therapeutic benefits of spinal orthotics?
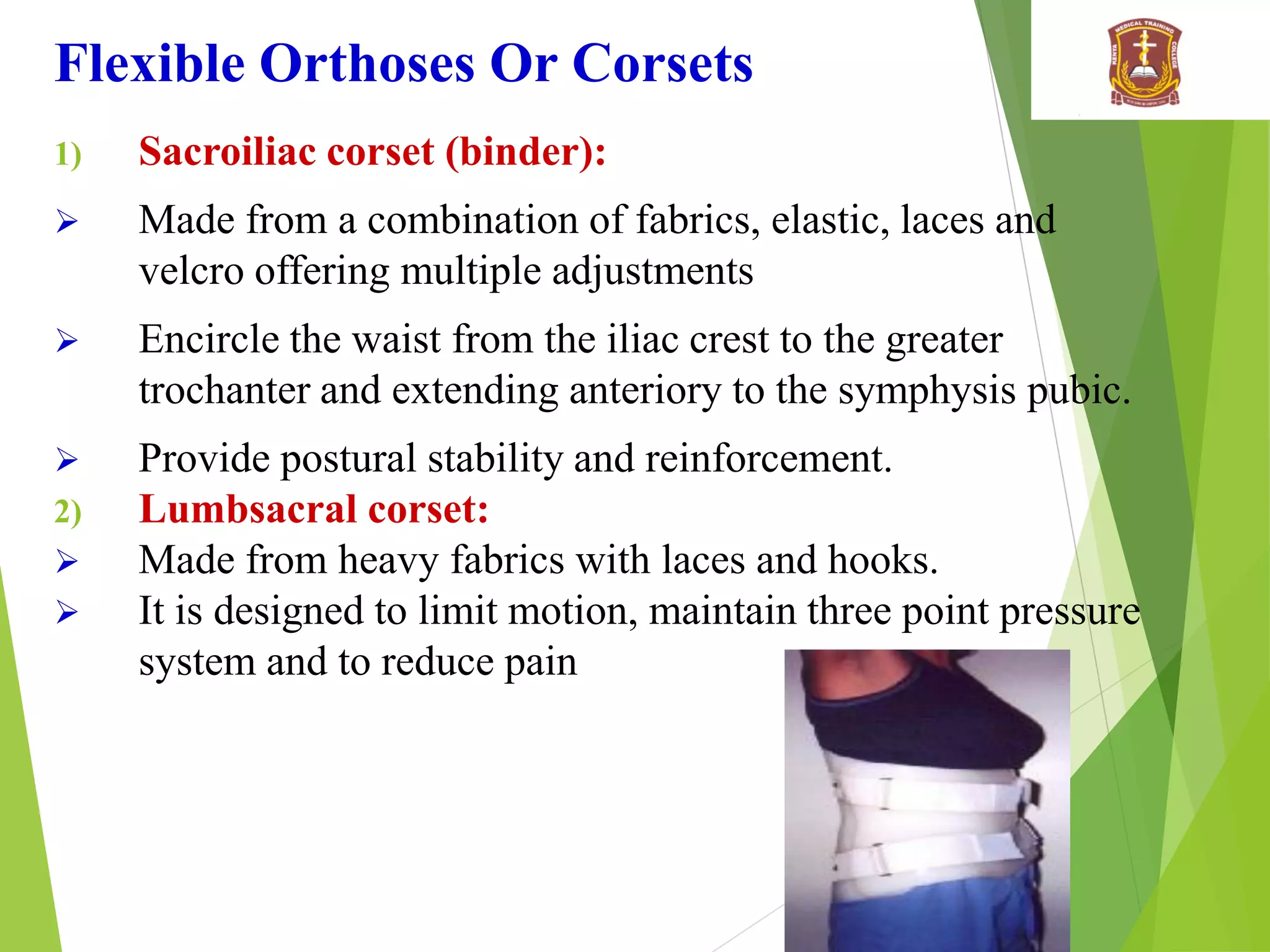
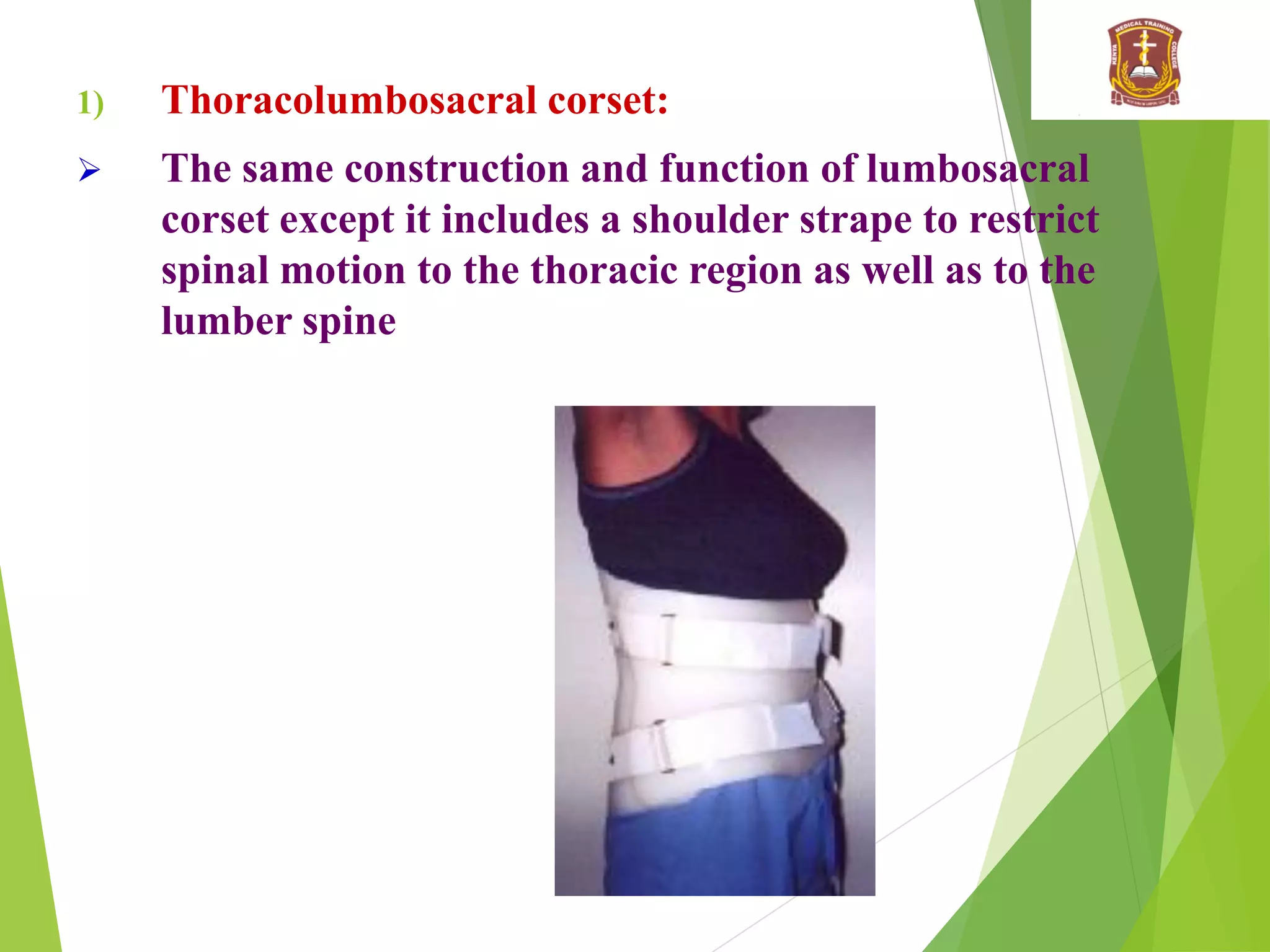
- How do flexible orthotics like corsets differ from rigid orthotics?
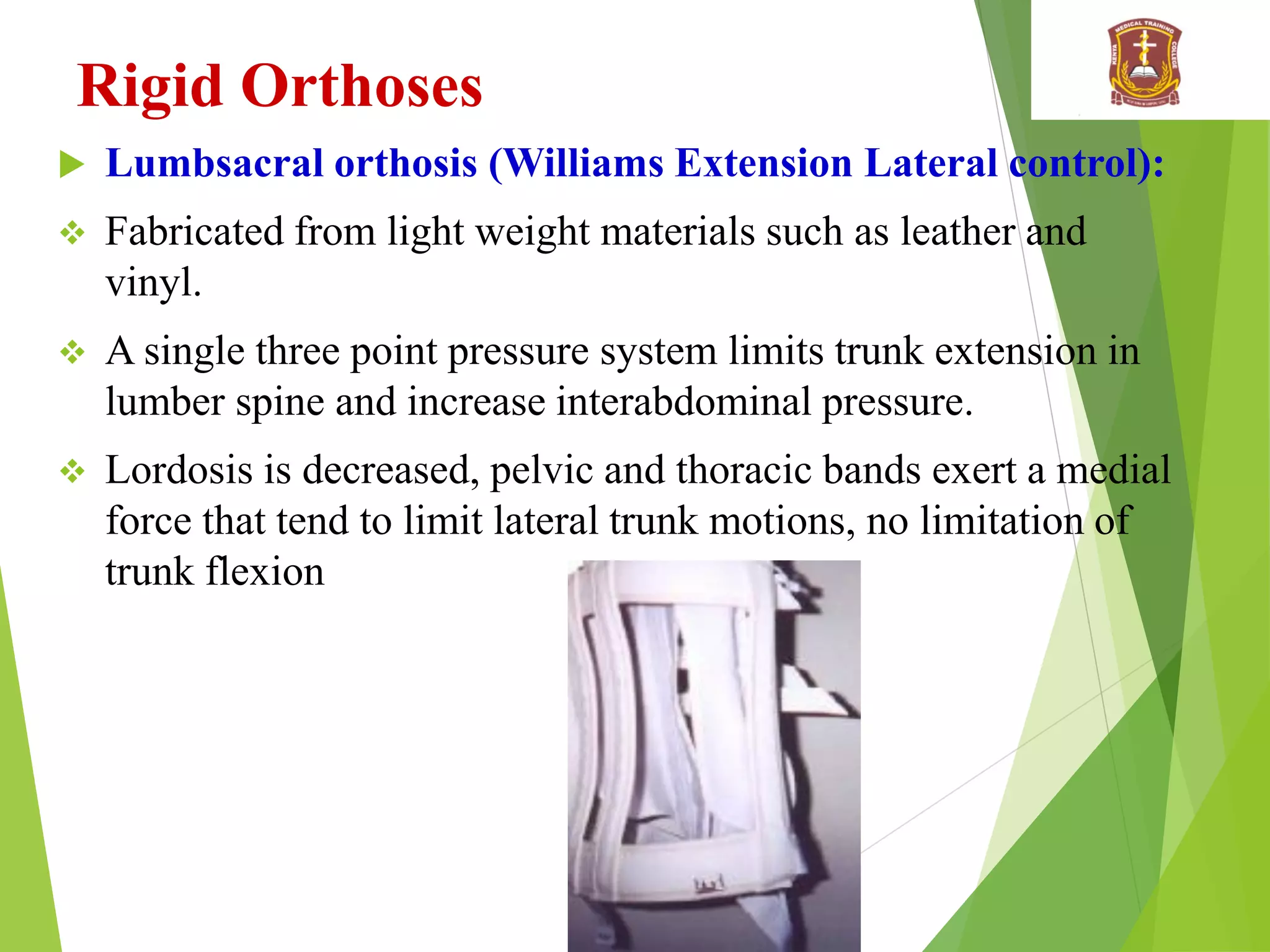
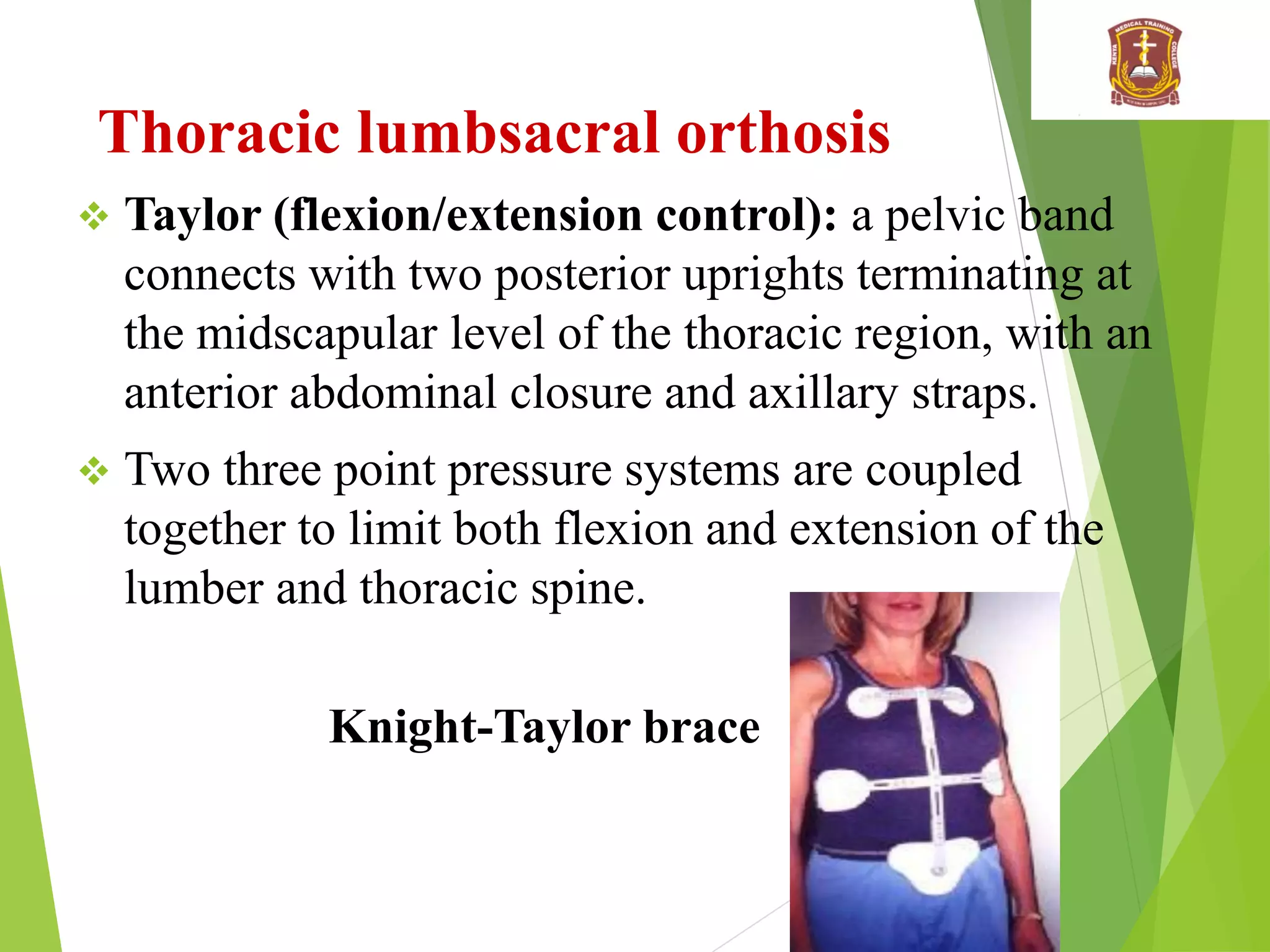
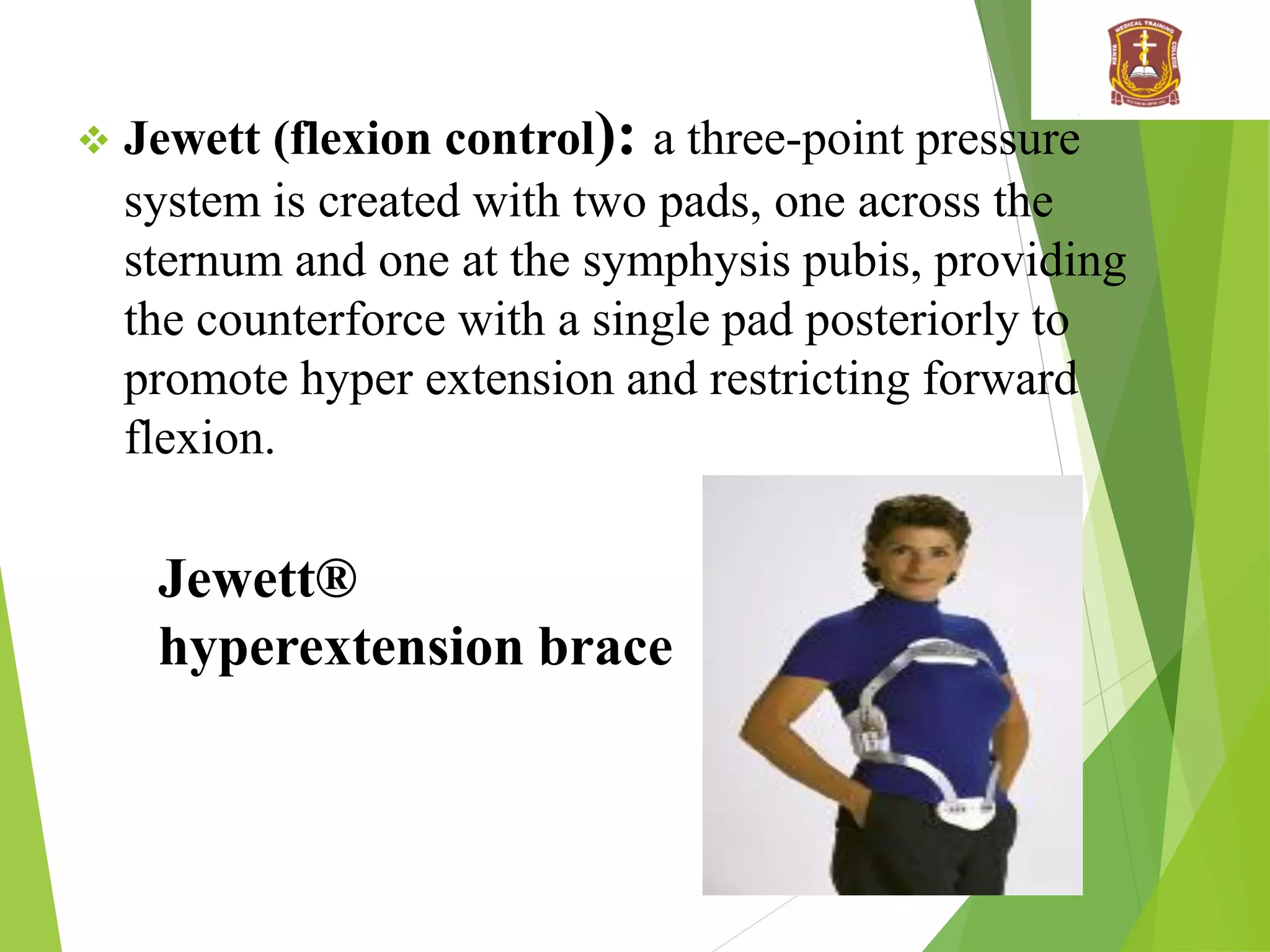
- What are some examples of rigid orthotics and what regions and motions do they restrict?
- What types of cervical orthotics are described ranging from soft to rigid?
- What is an example of a cervicothoraciclumbosacral orthosis and what region does it restrict?
![Cervicothoracic Orthoses
3- Sterno-occipital mandibullar immobilizer [SOMI]
Is one of the most common post surgical appliances
It consists of a rigid metal frame with a chin and occipital rest
connected to a chest and back plate, with padded shoulder and
trunk straps.
The added chest and back plates help to reduce cervical
motion by an average of 55 to 75 percent.
Sternooccipital-
mandibular
immobilization
brace](https://image.slidesharecdn.com/spineorthotics-1-230622174651-e51d27e8/75/Spine-Orthotics-1-pdf-18-2048.jpg)