This document provides an overview of radial head and neck fractures, including anatomy, classification, treatment options, and surgical approaches. Key points include:
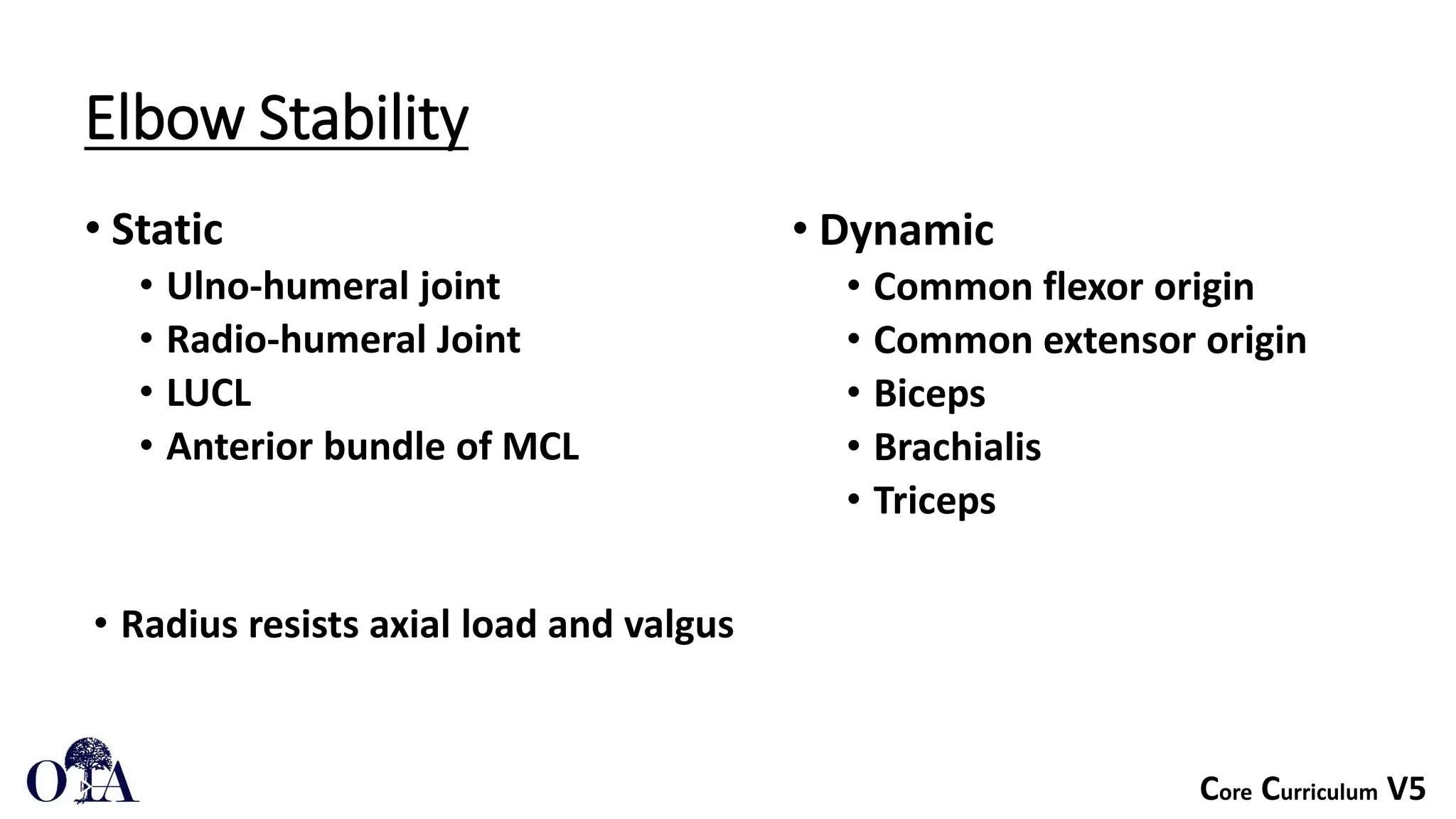
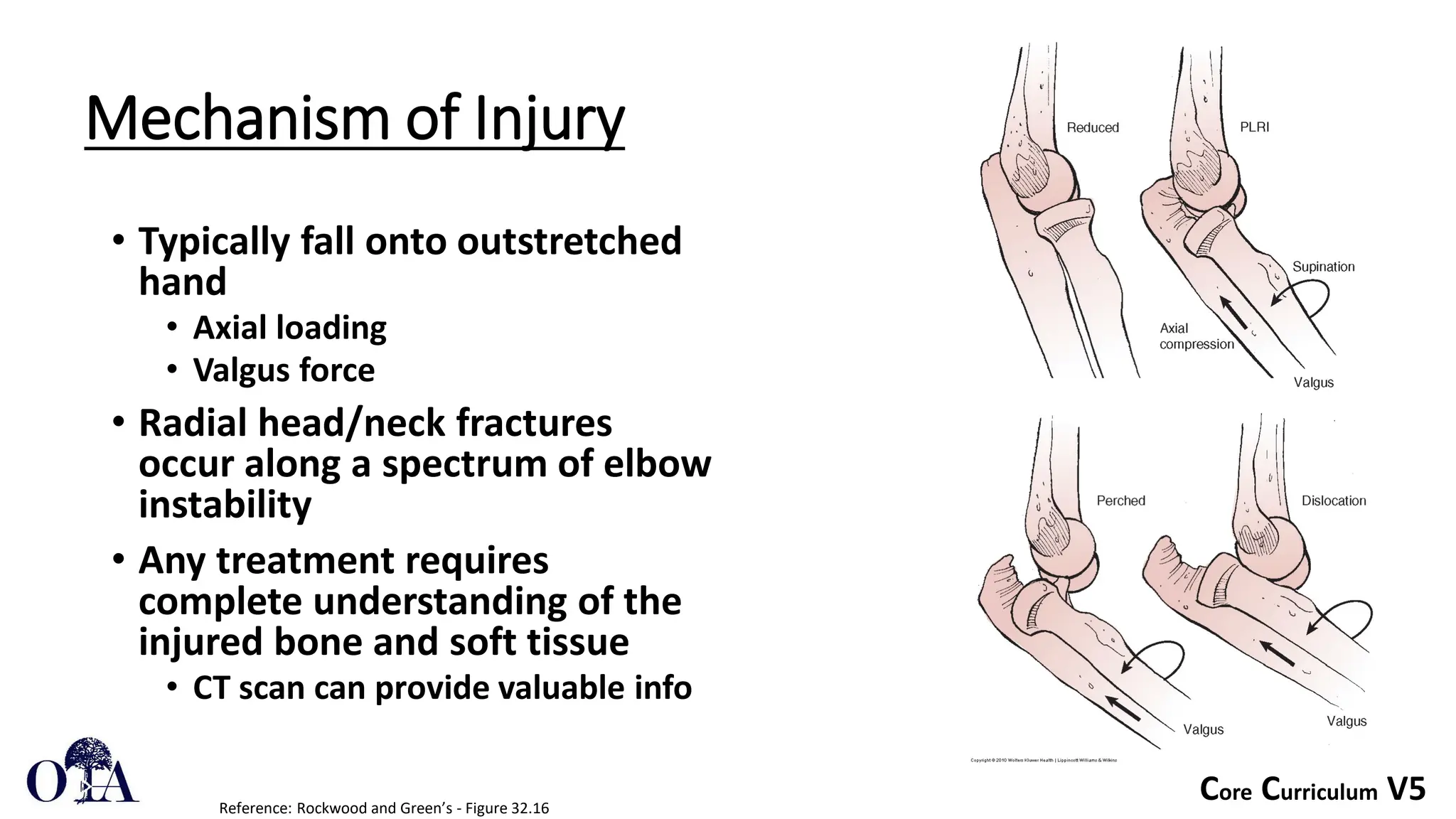
- Radial head and neck fractures are typically caused by a fall onto an outstretched hand, resulting in axial loading and valgus force.
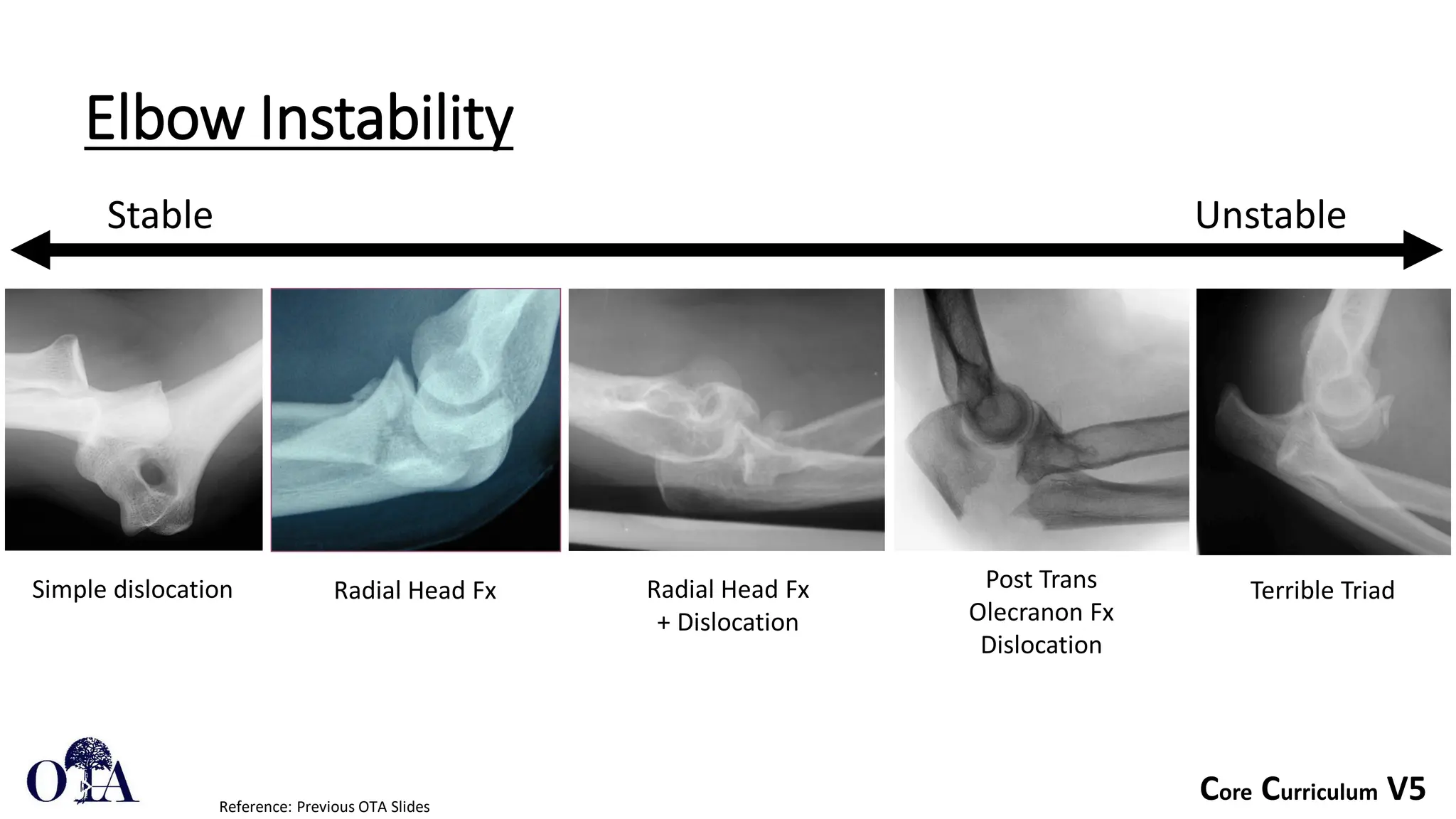
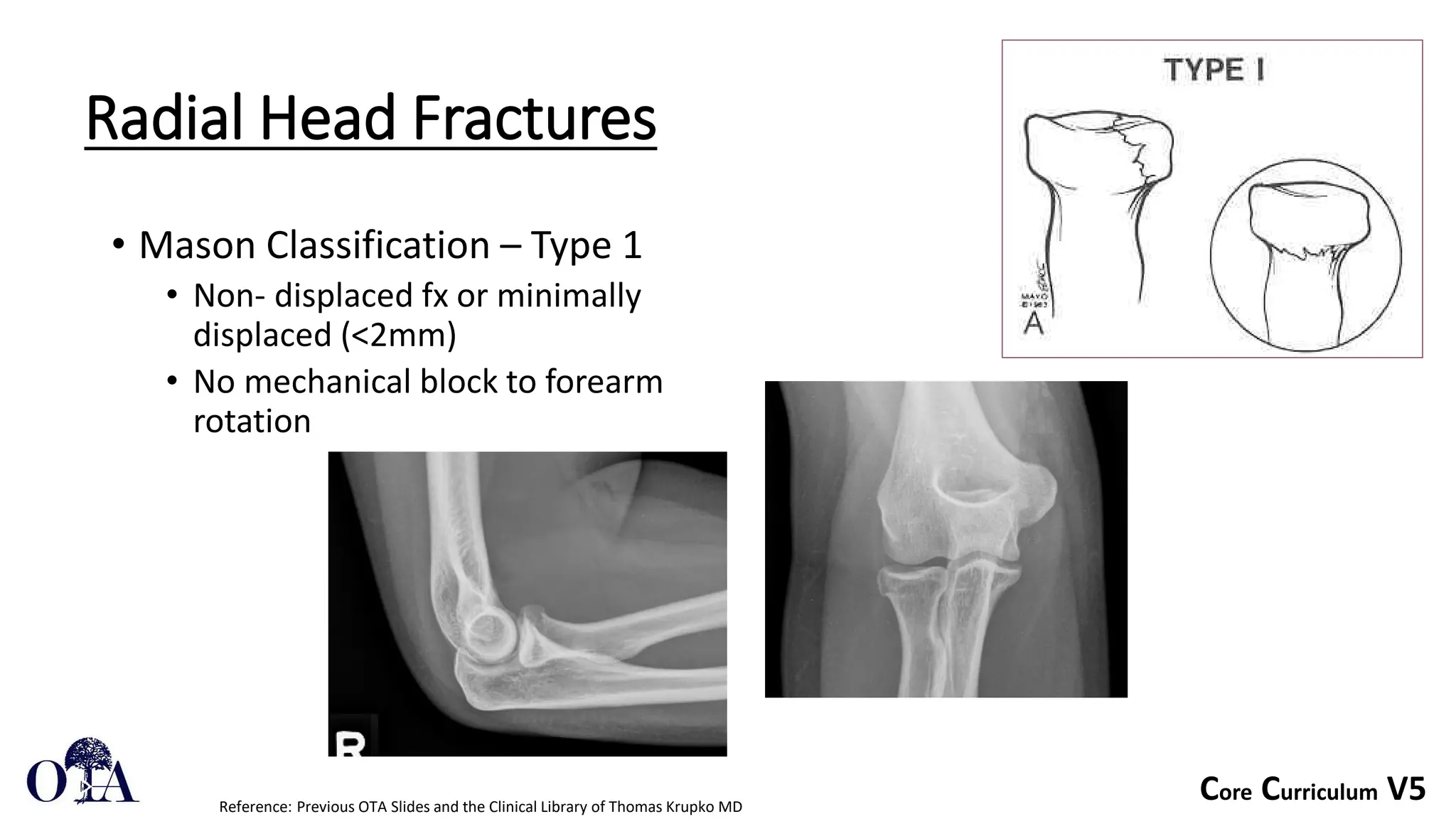
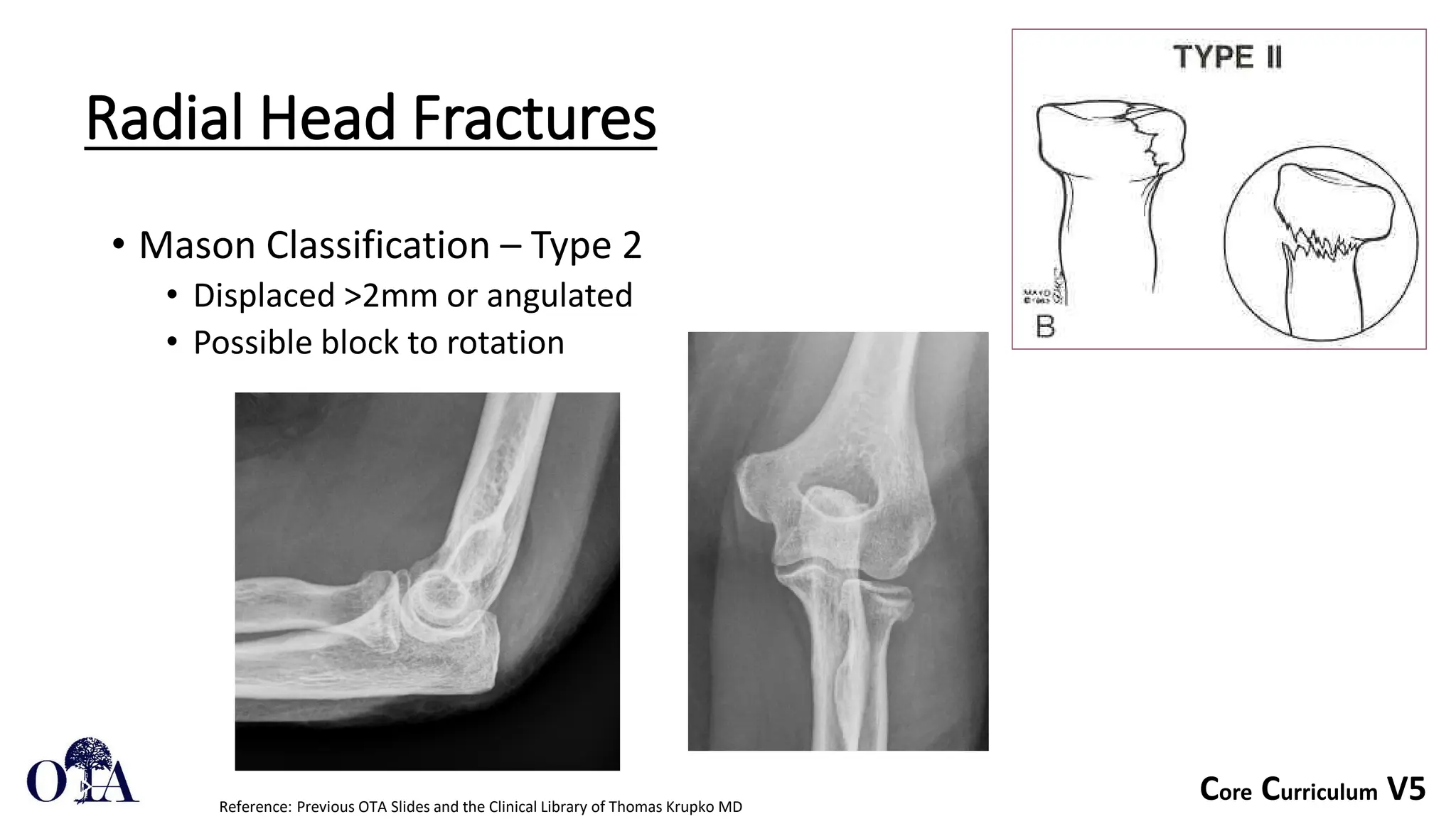
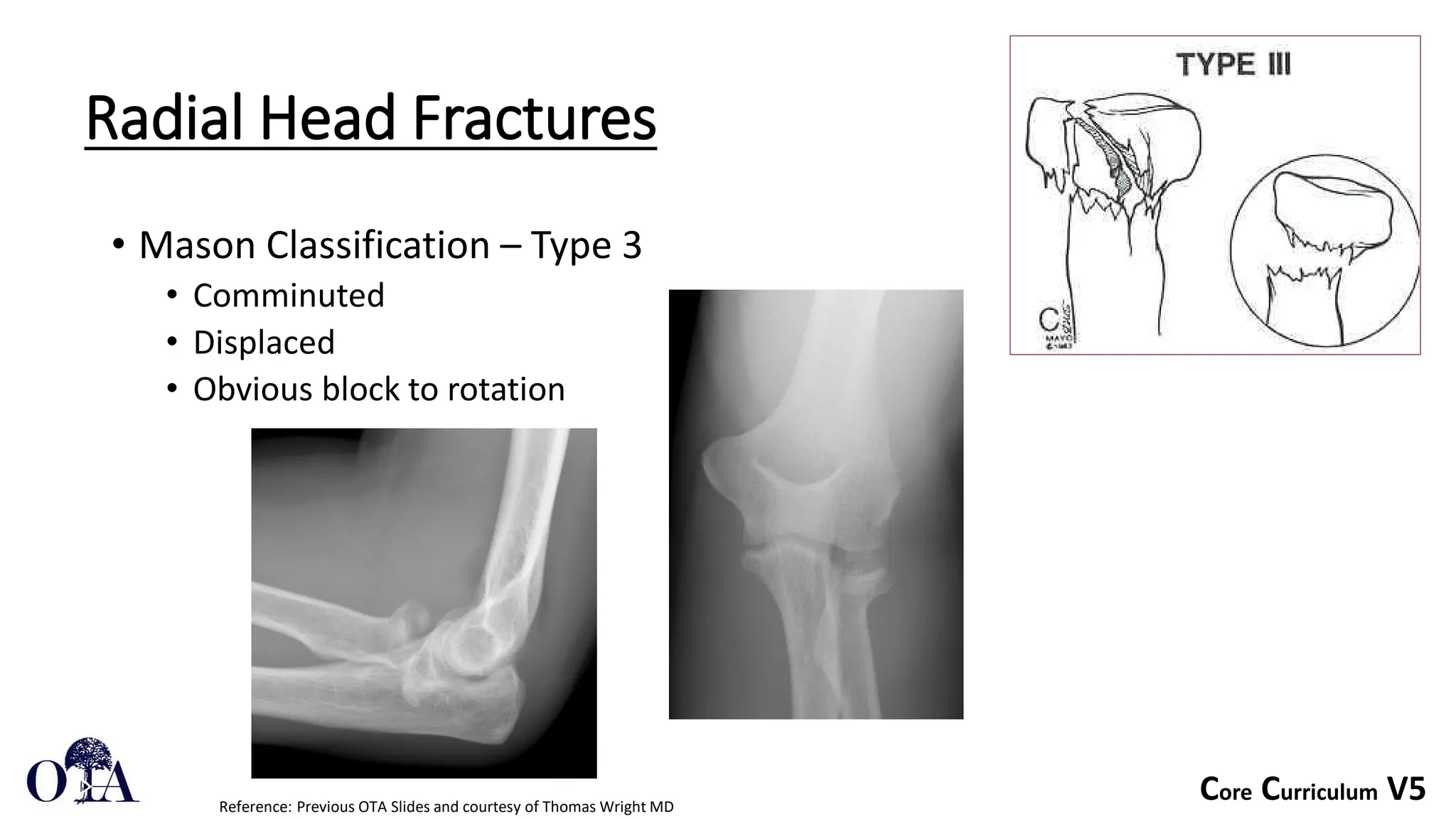
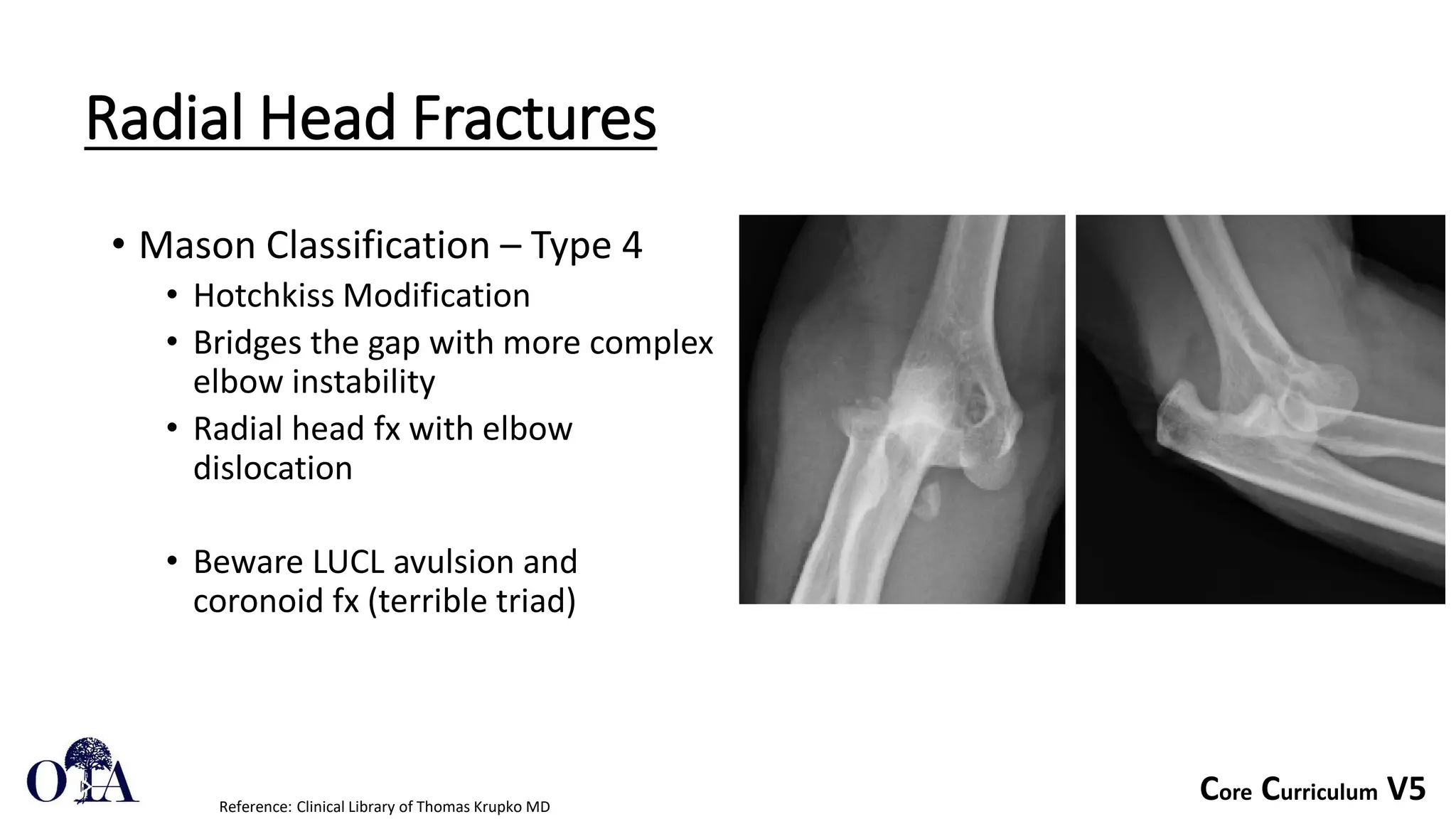
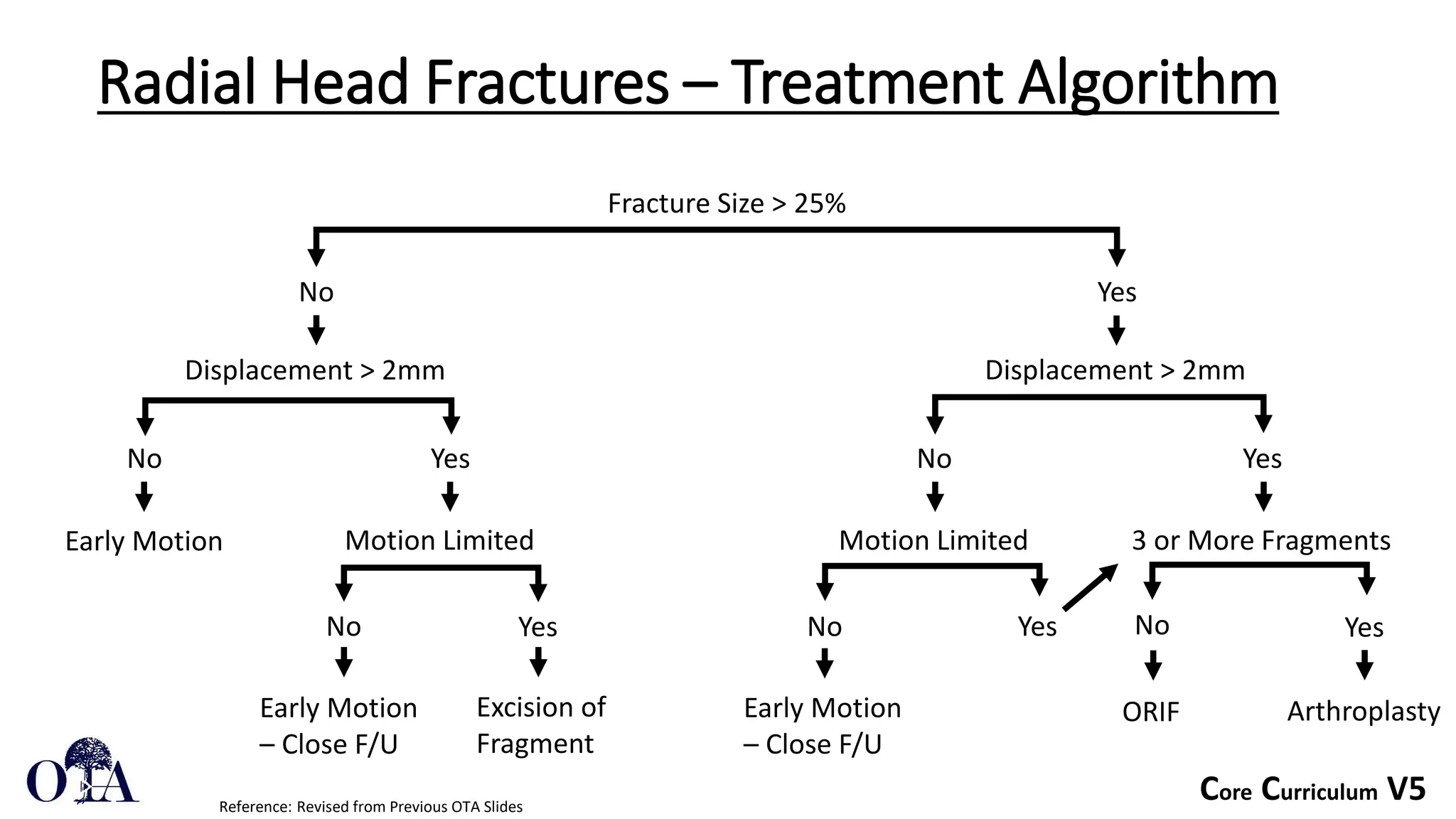
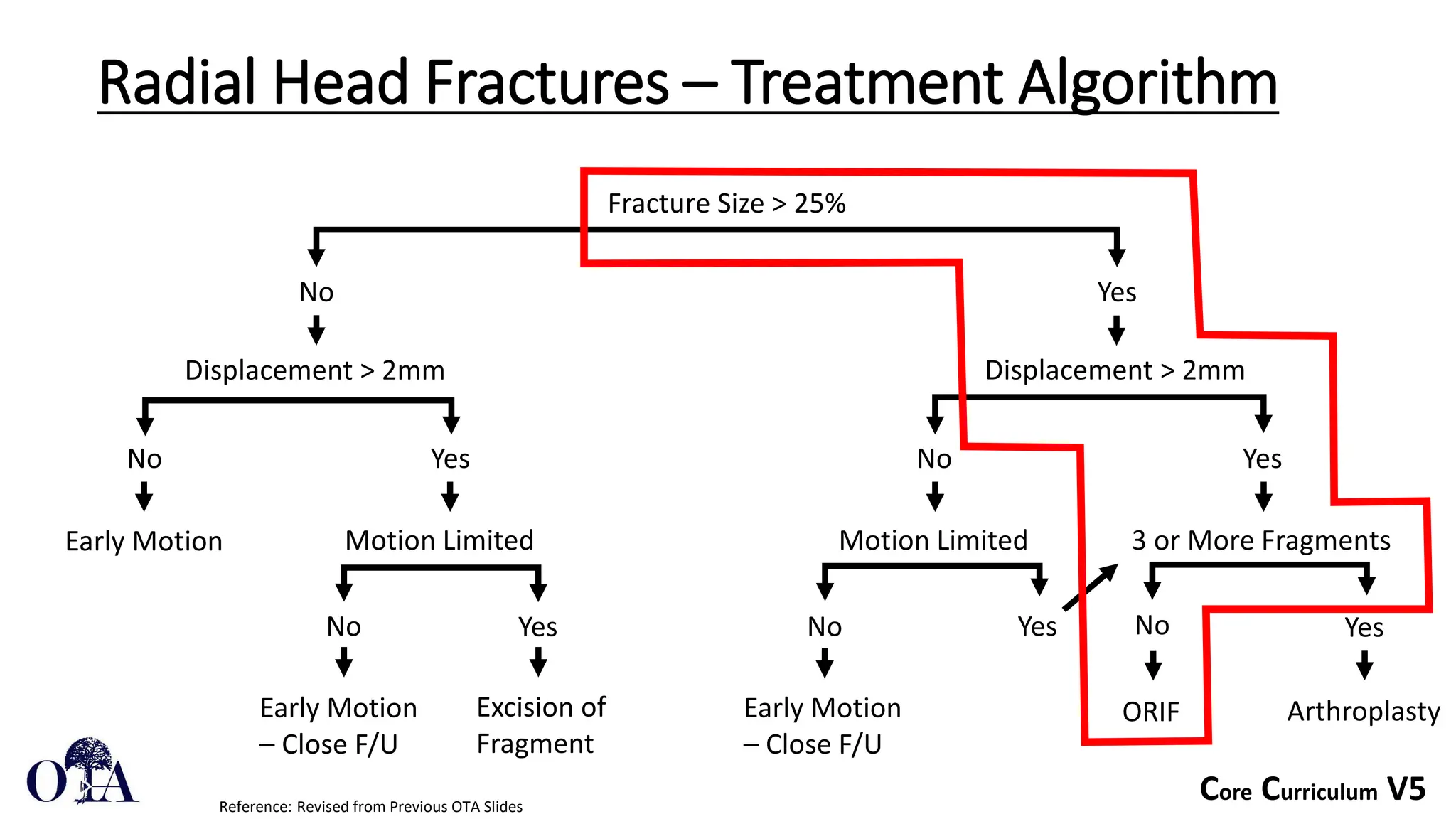
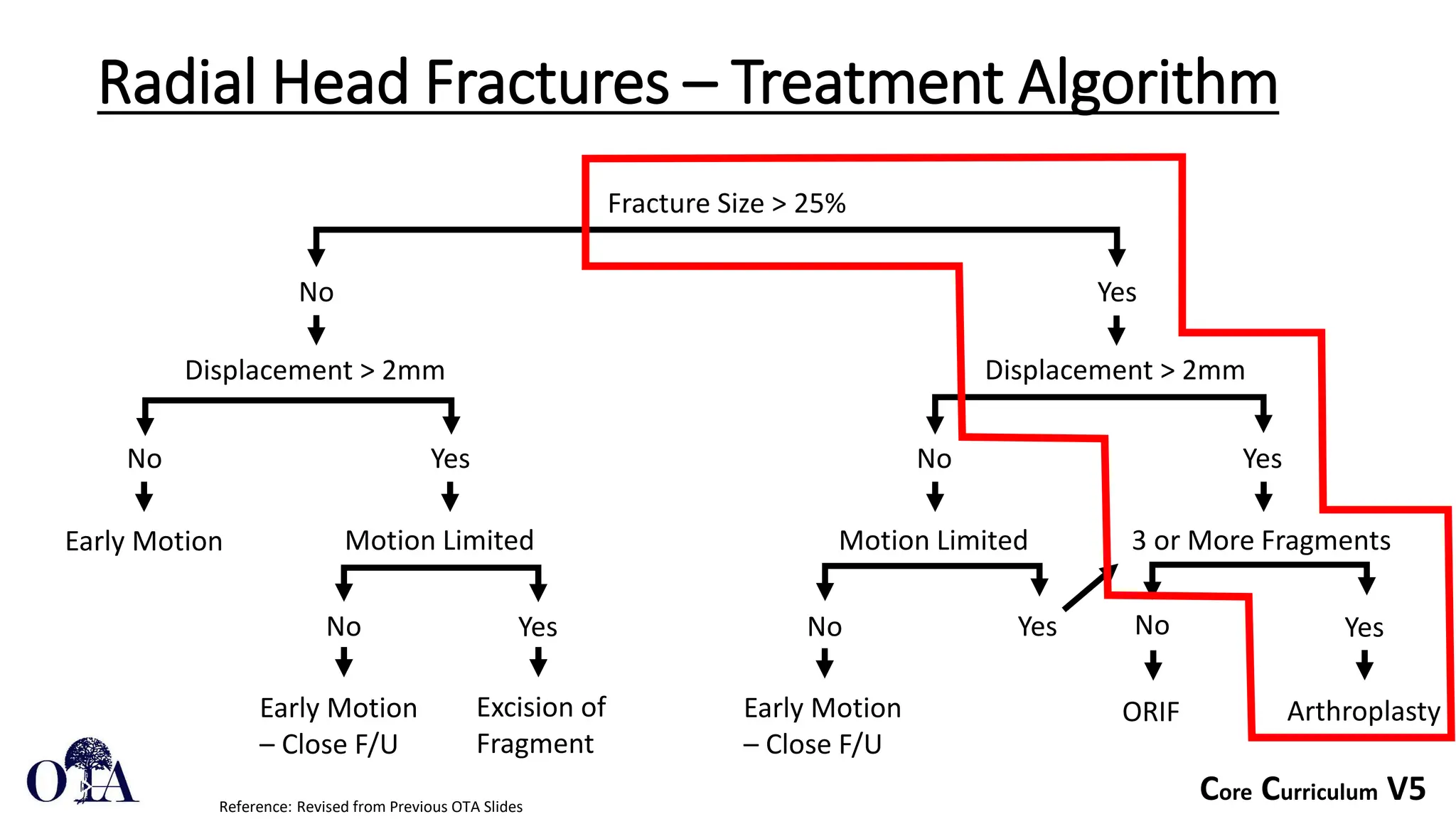
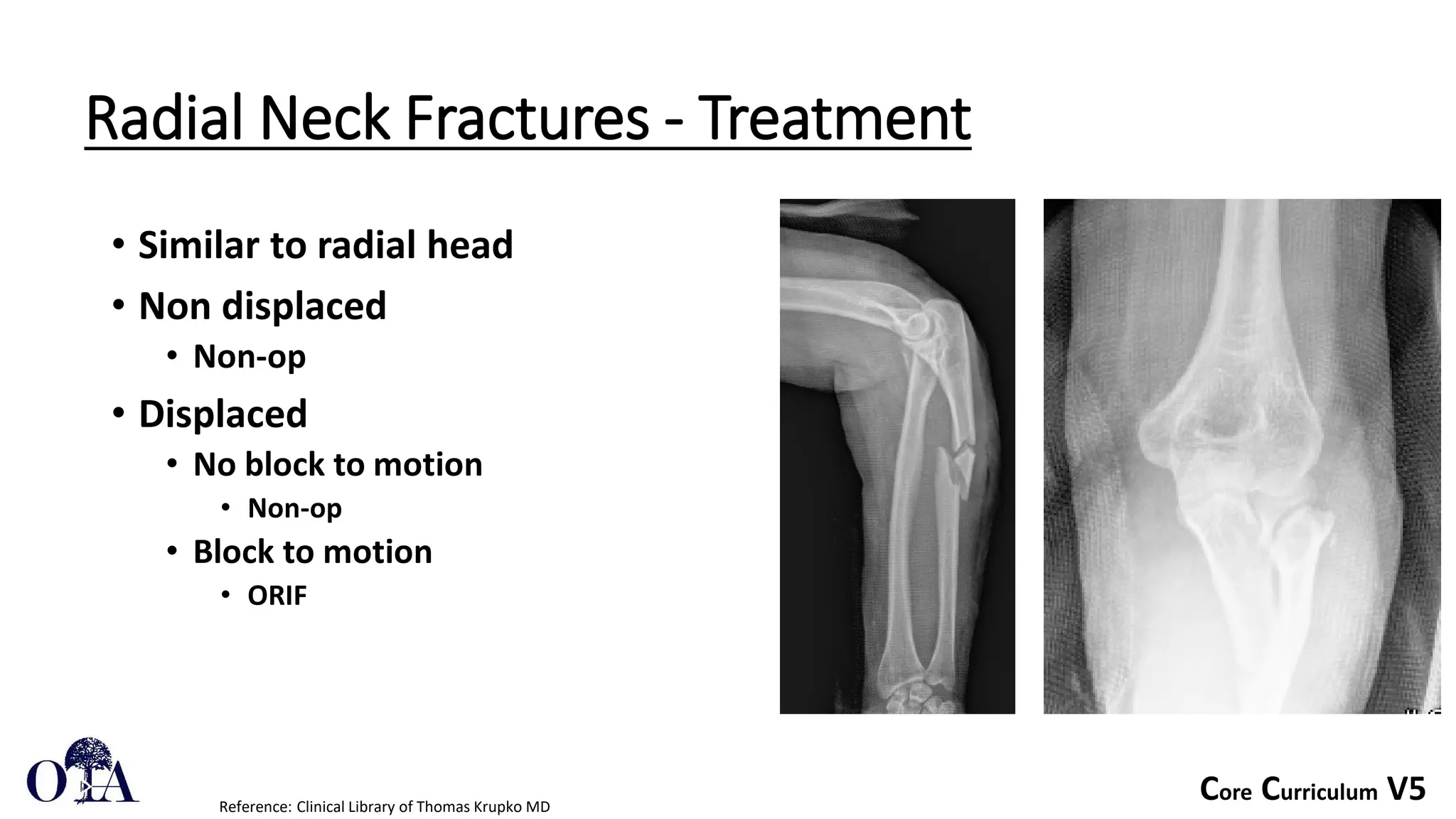
- Fractures are classified using the Mason system from non-displaced to comminuted. Treatment depends on displacement and stability.
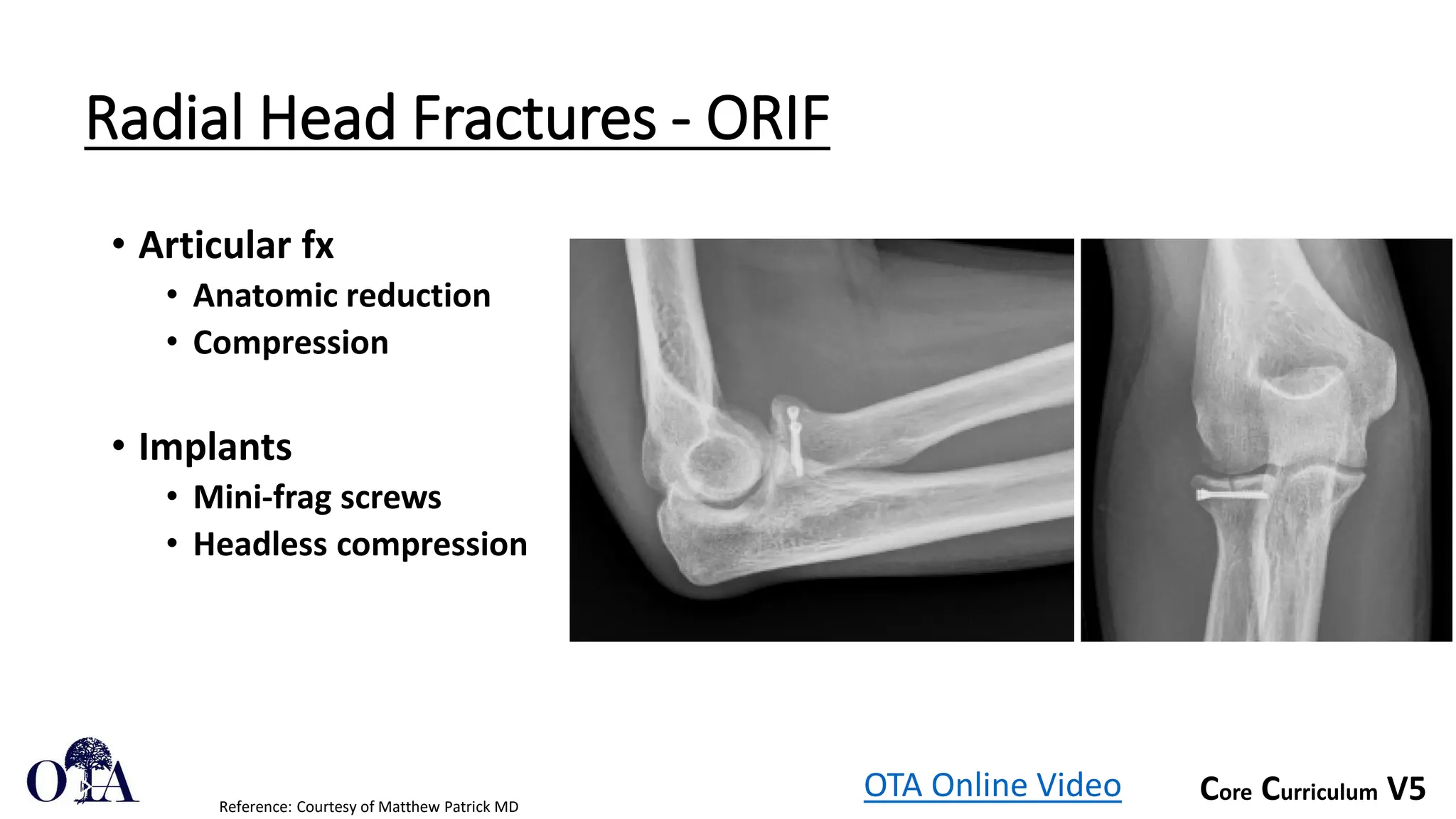
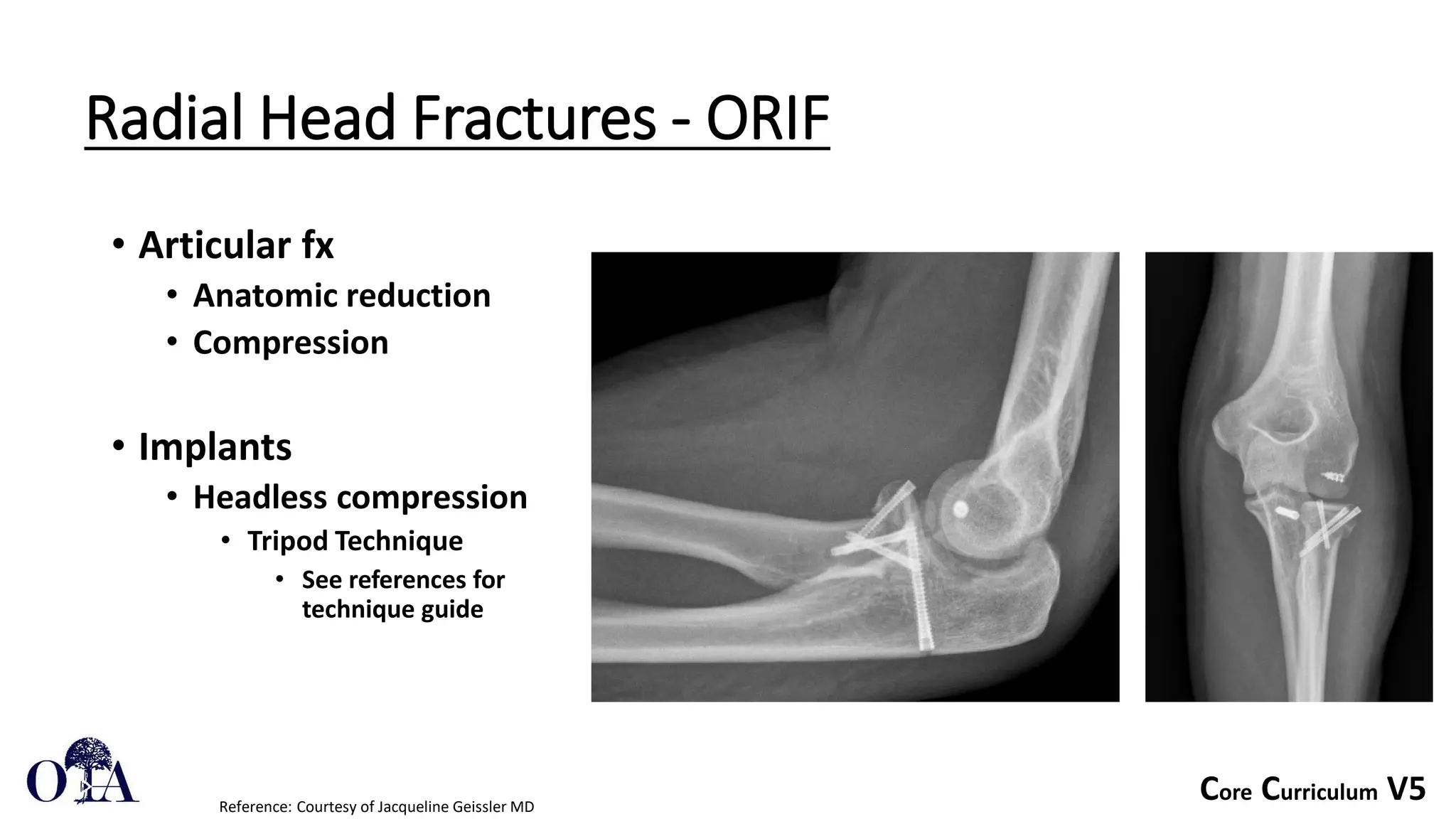
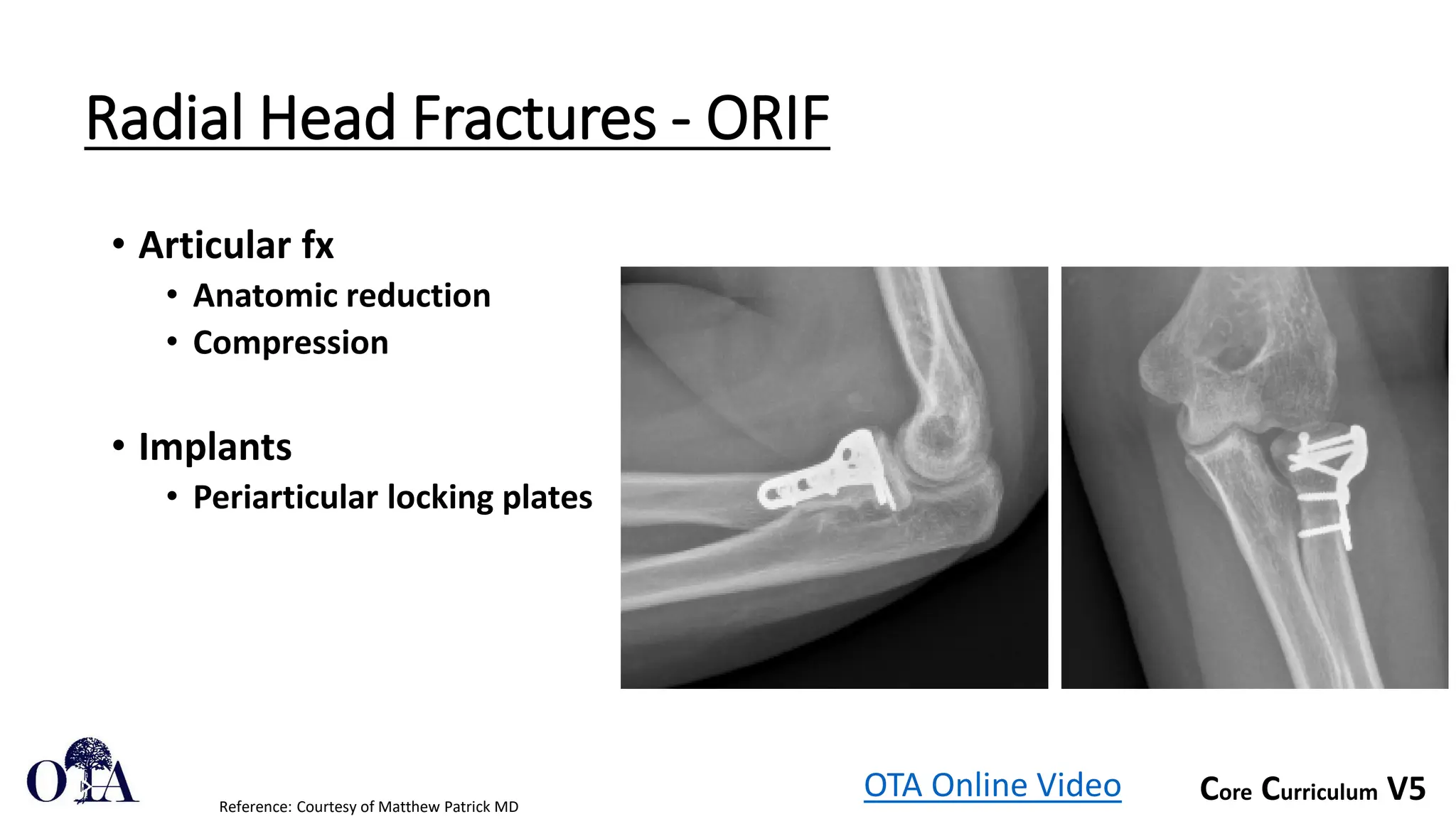
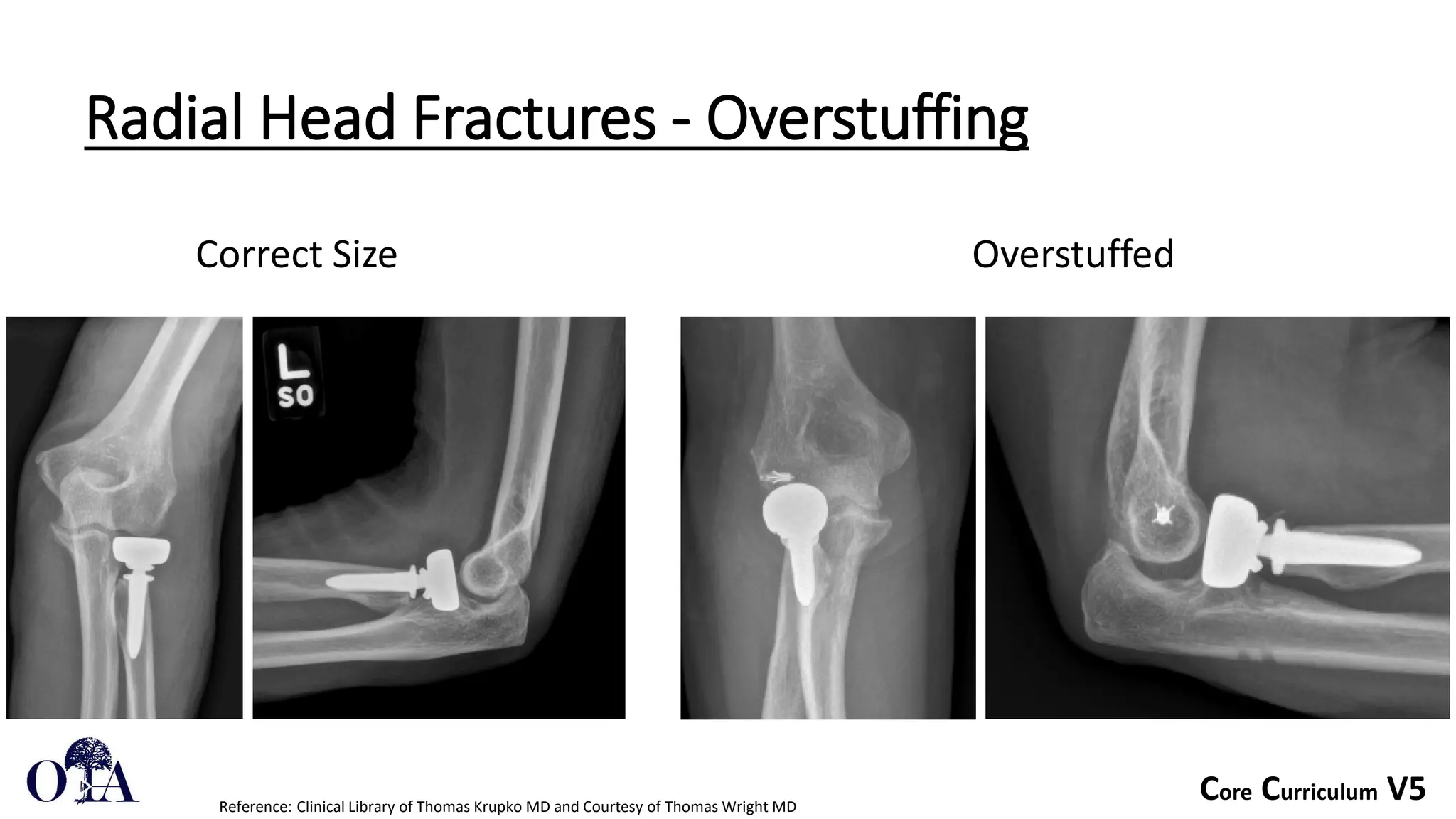
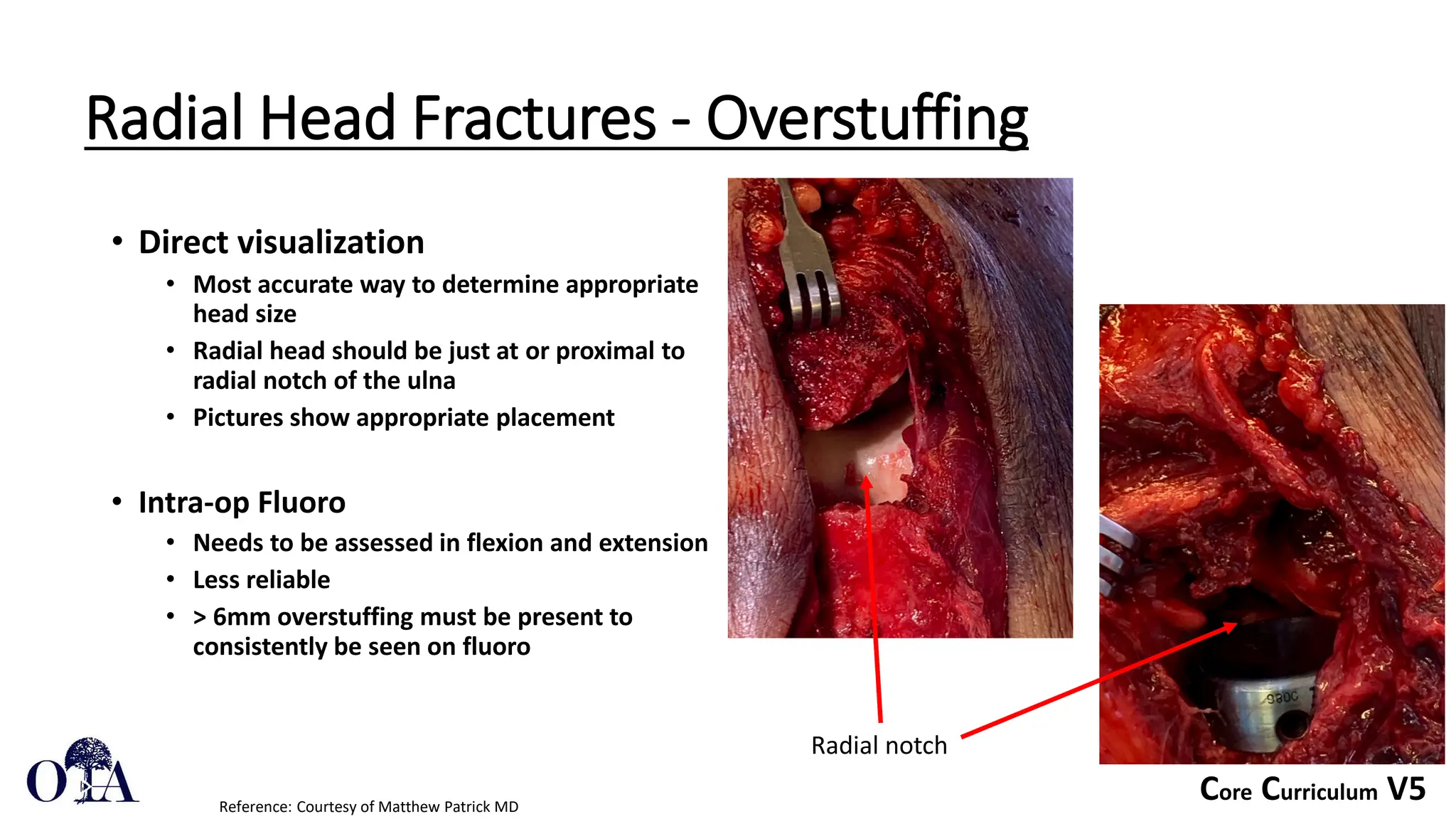
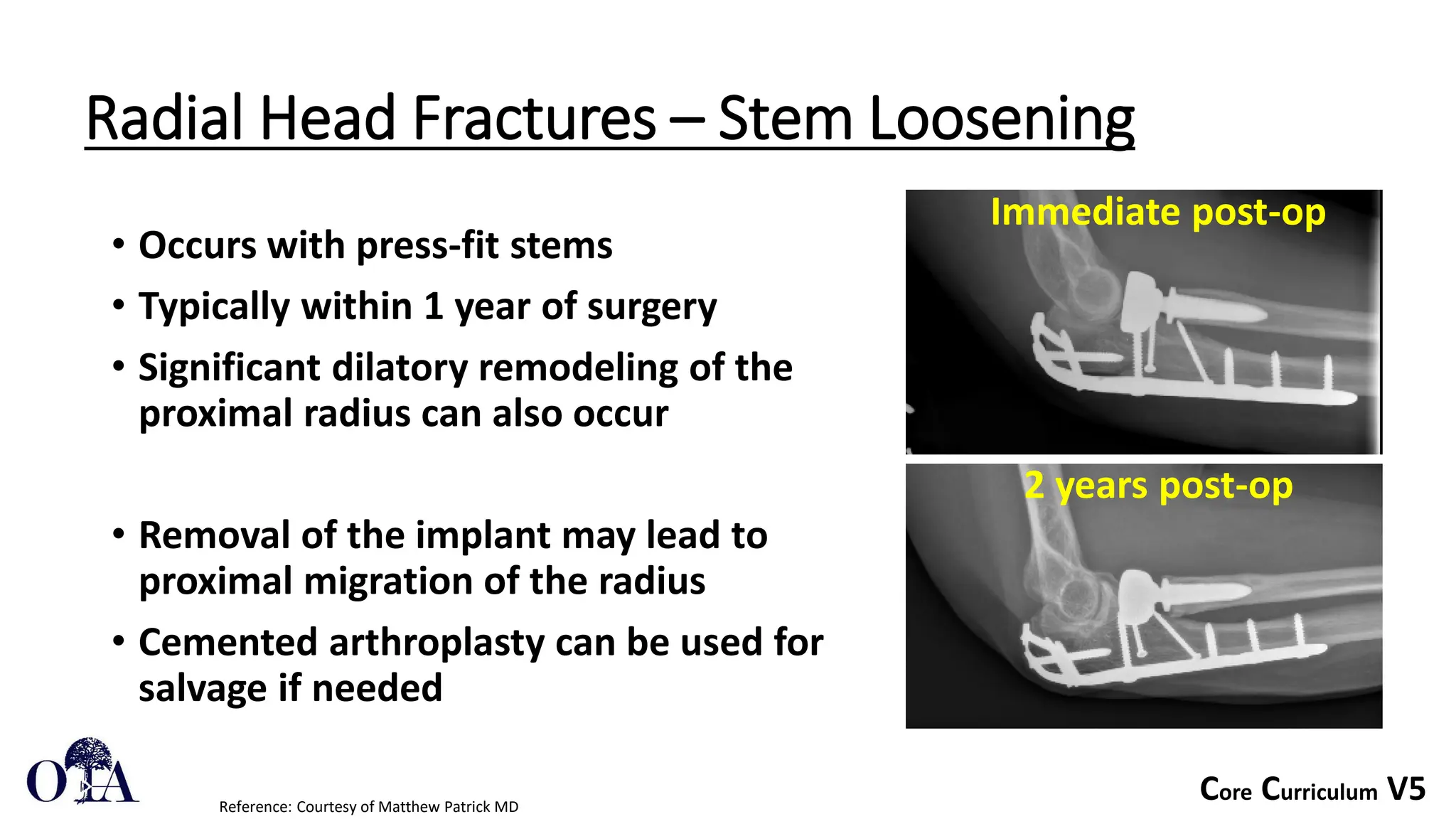
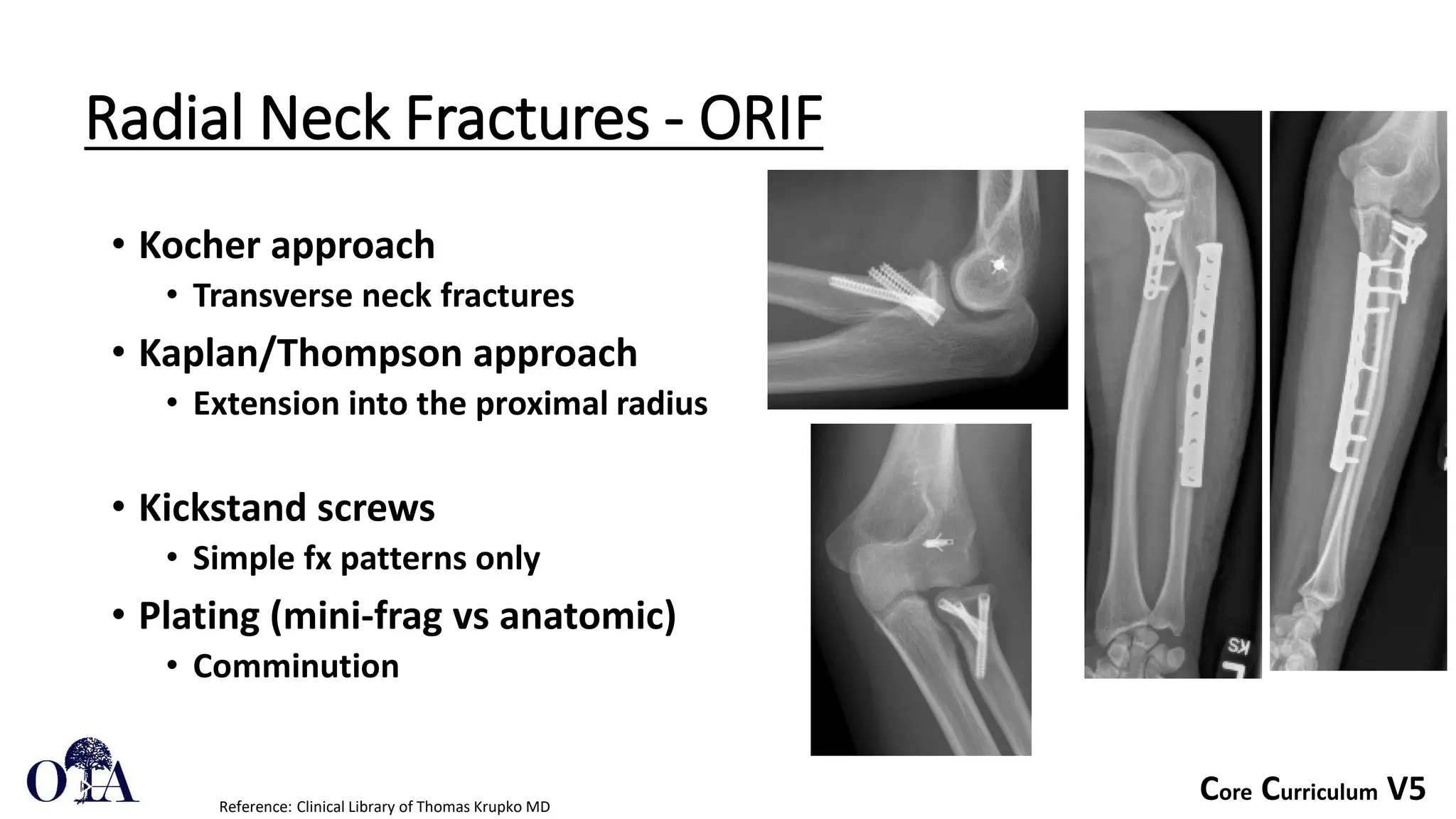
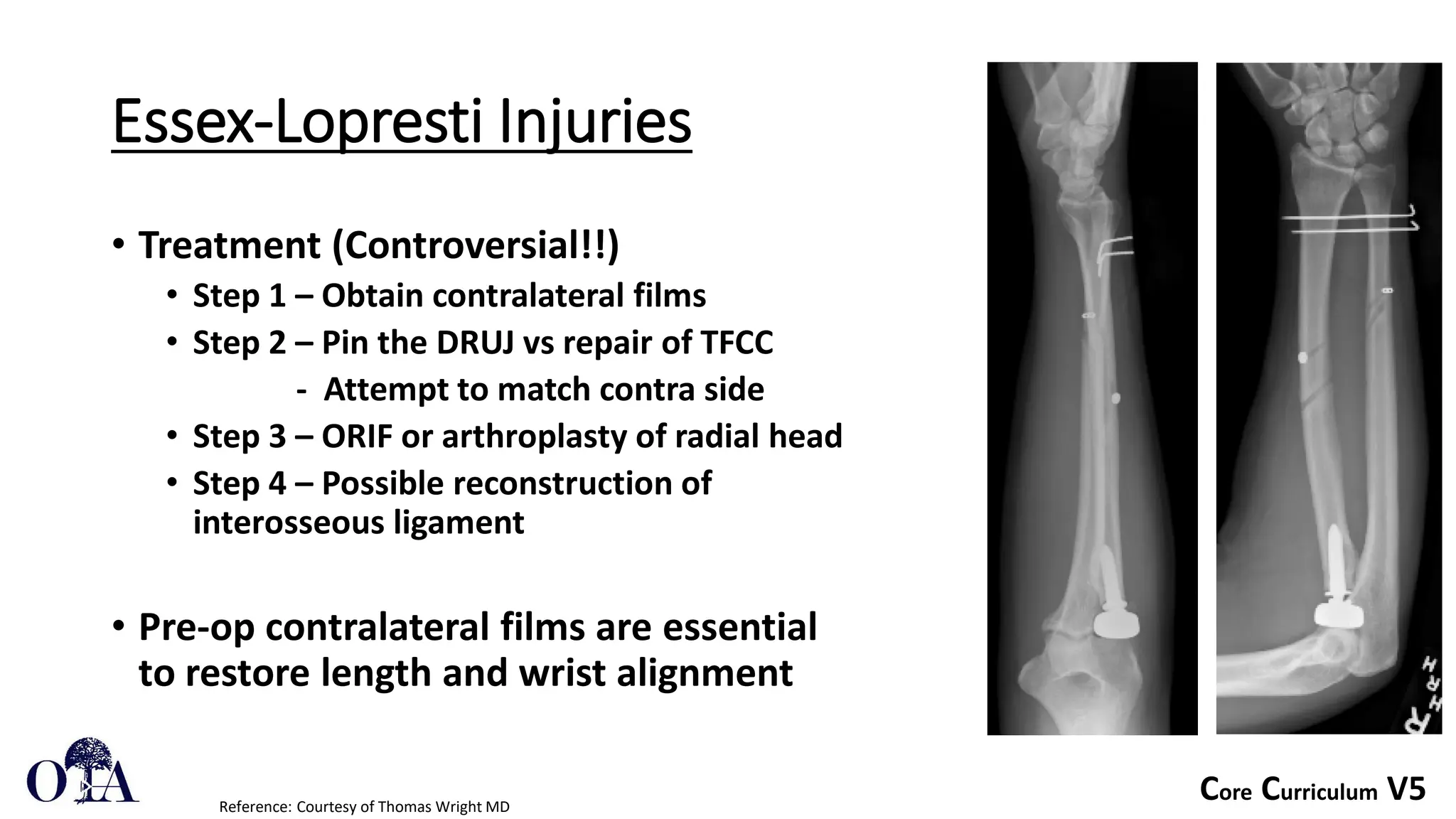
- Surgical options include excision of fragments, open reduction and internal fixation, or radial head arthroplasty. Placement of implants and sizing of replacements is important to avoid complications.
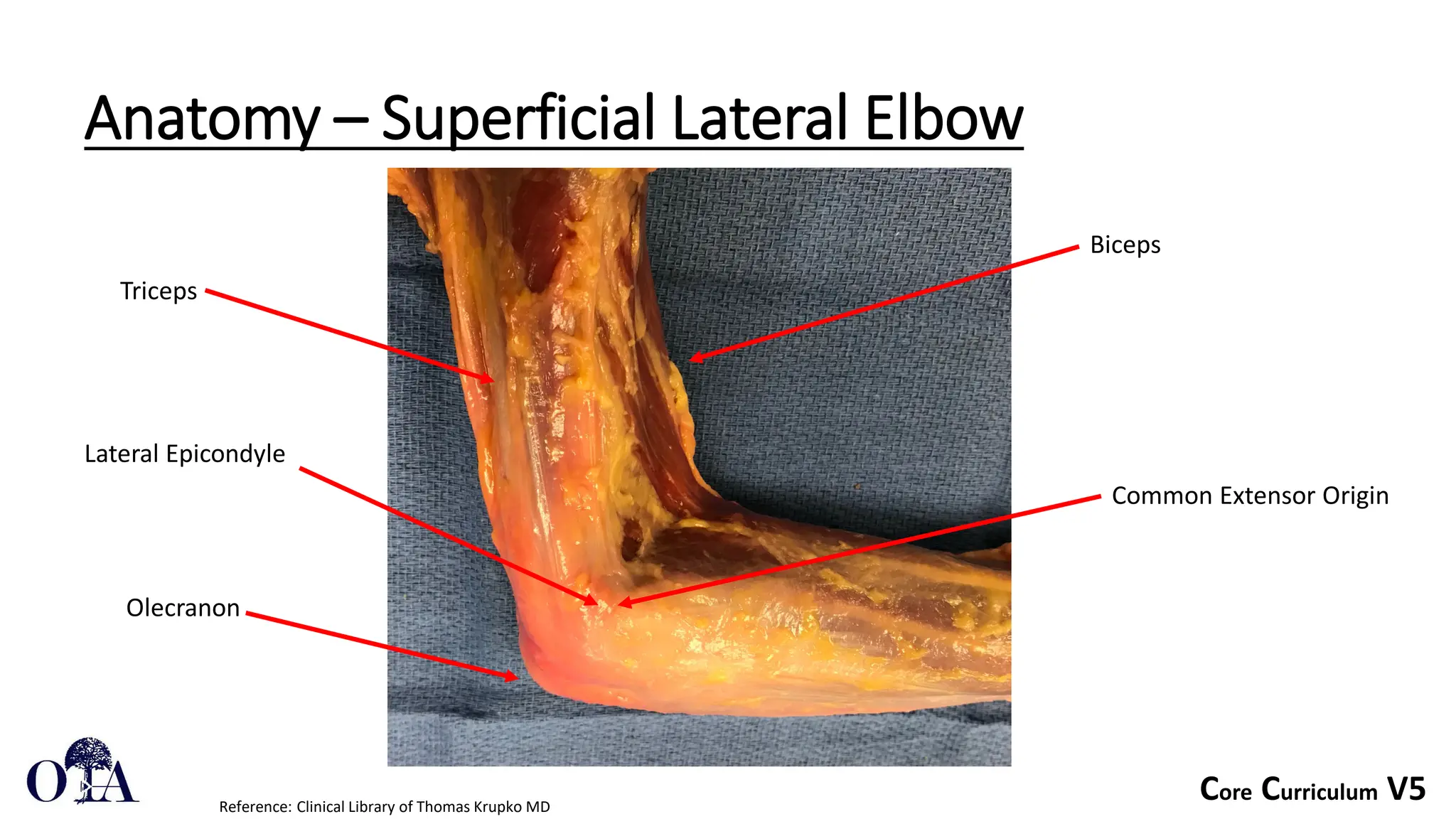
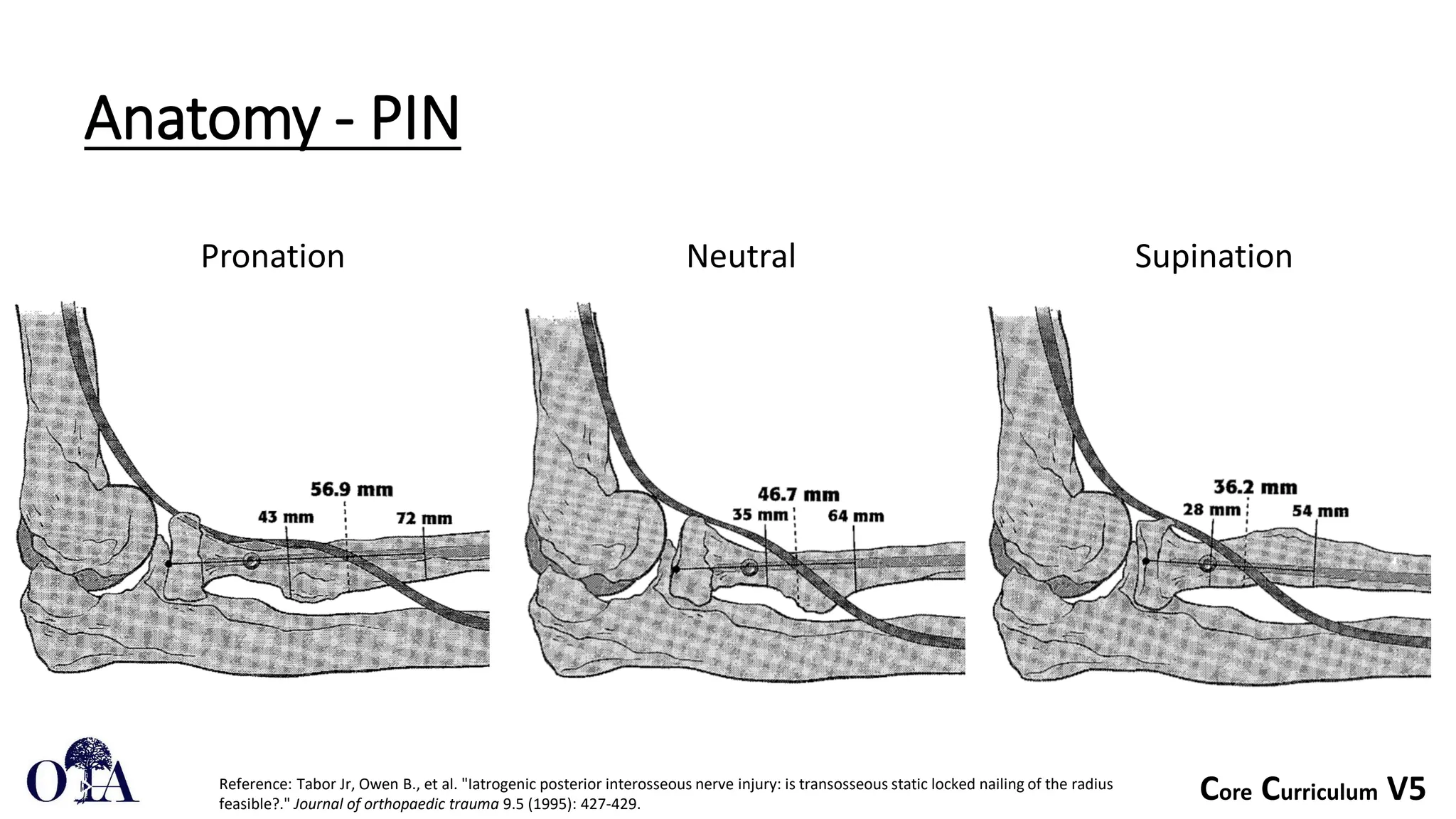
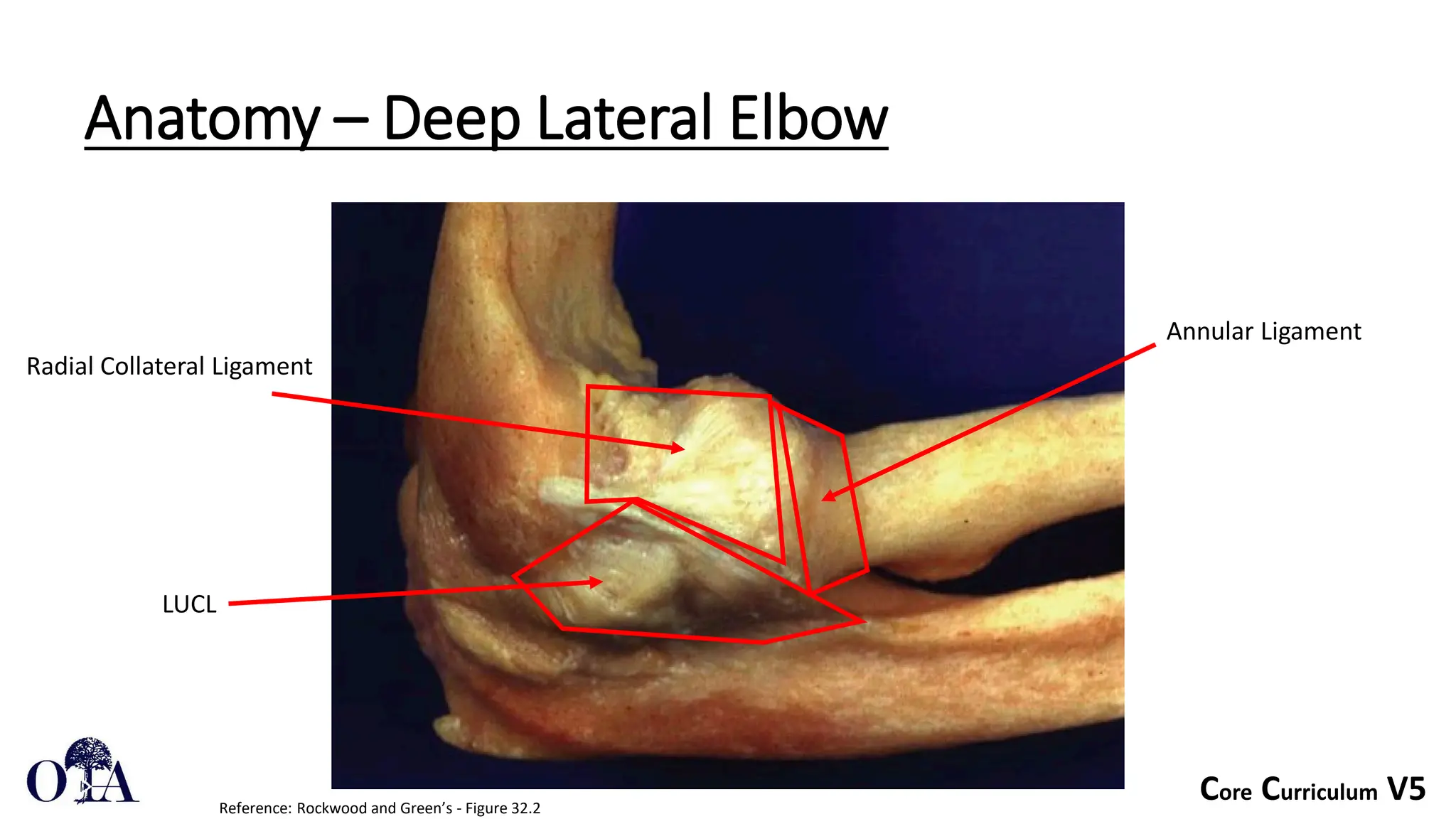
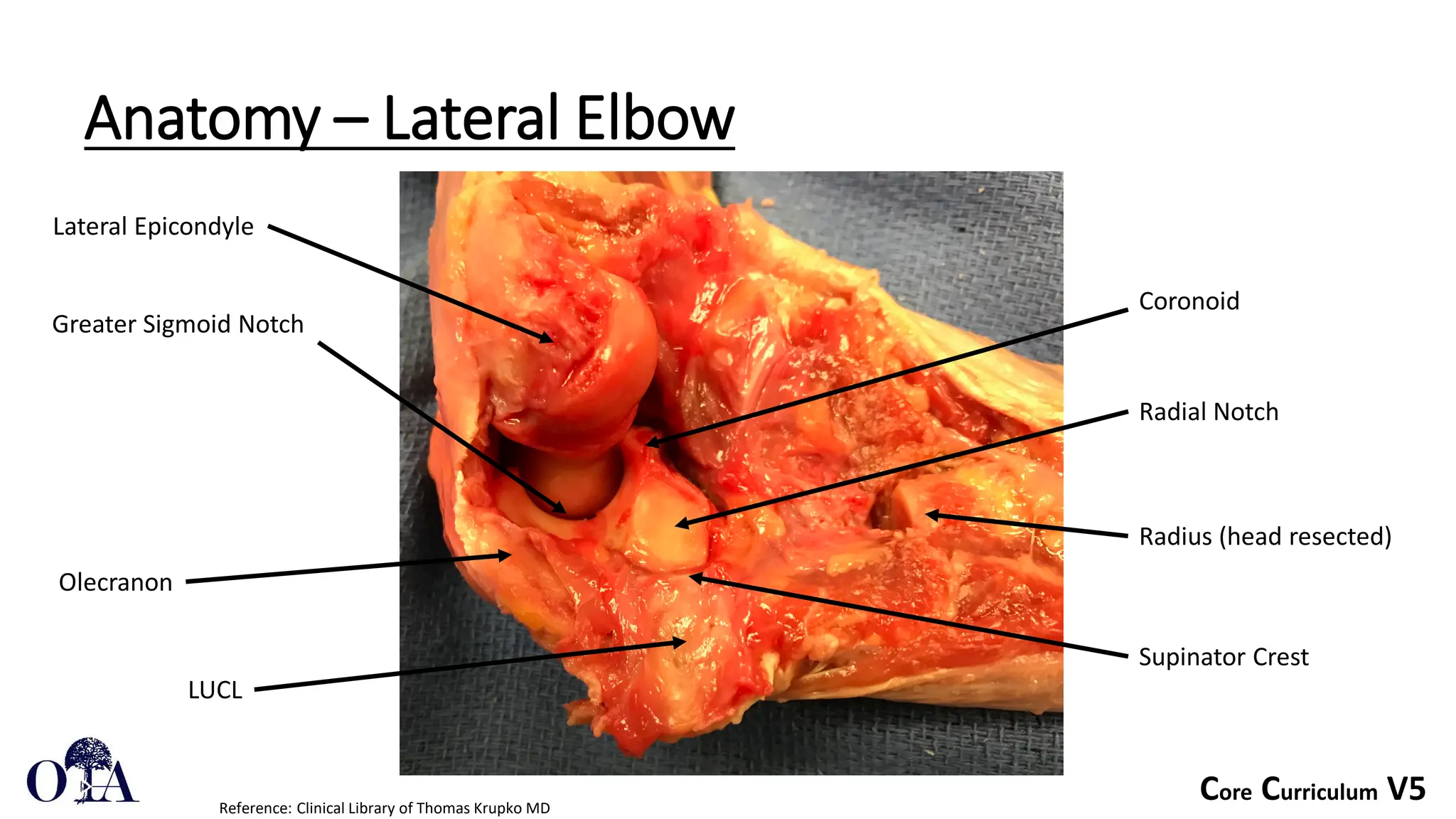
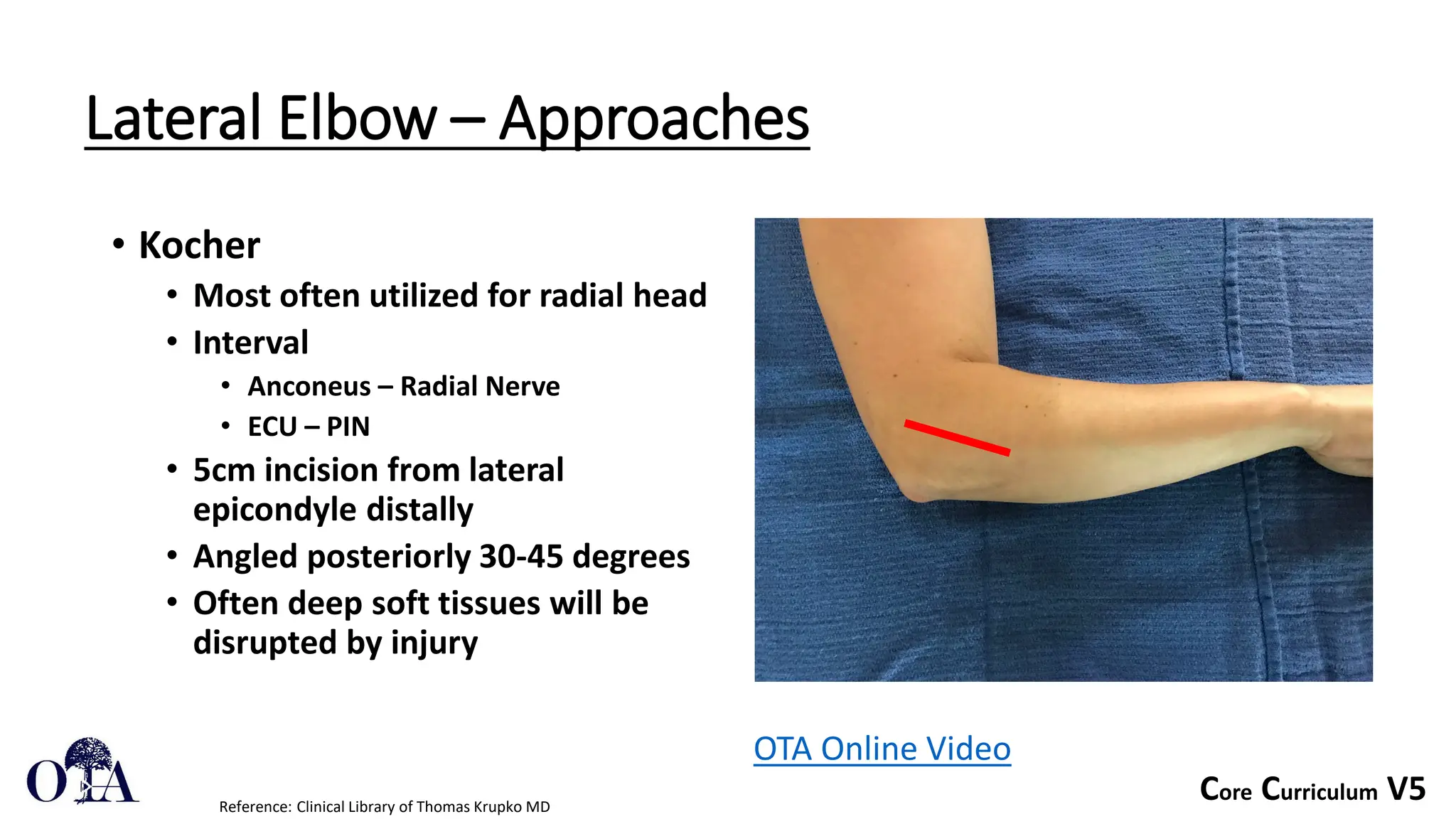
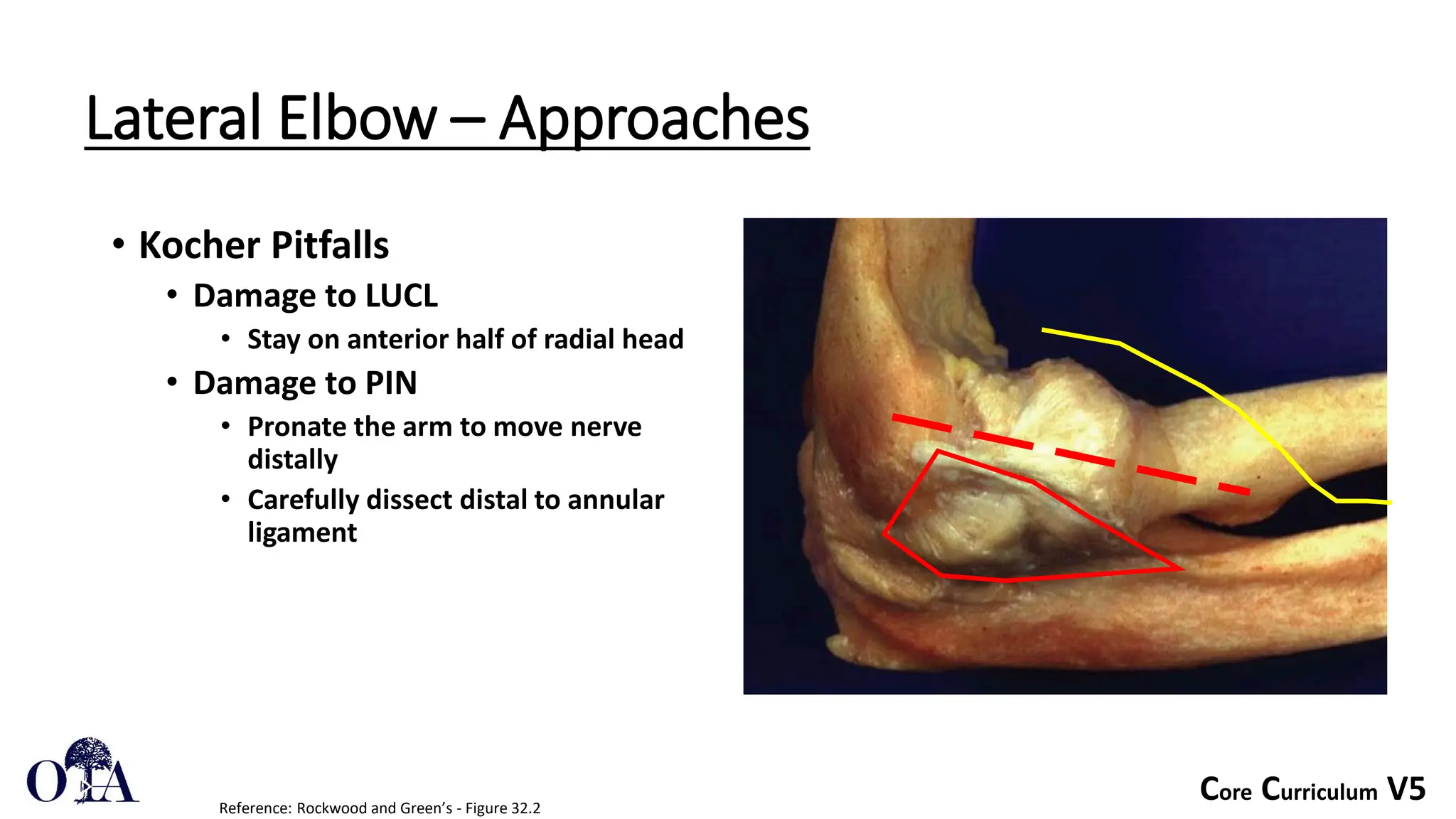
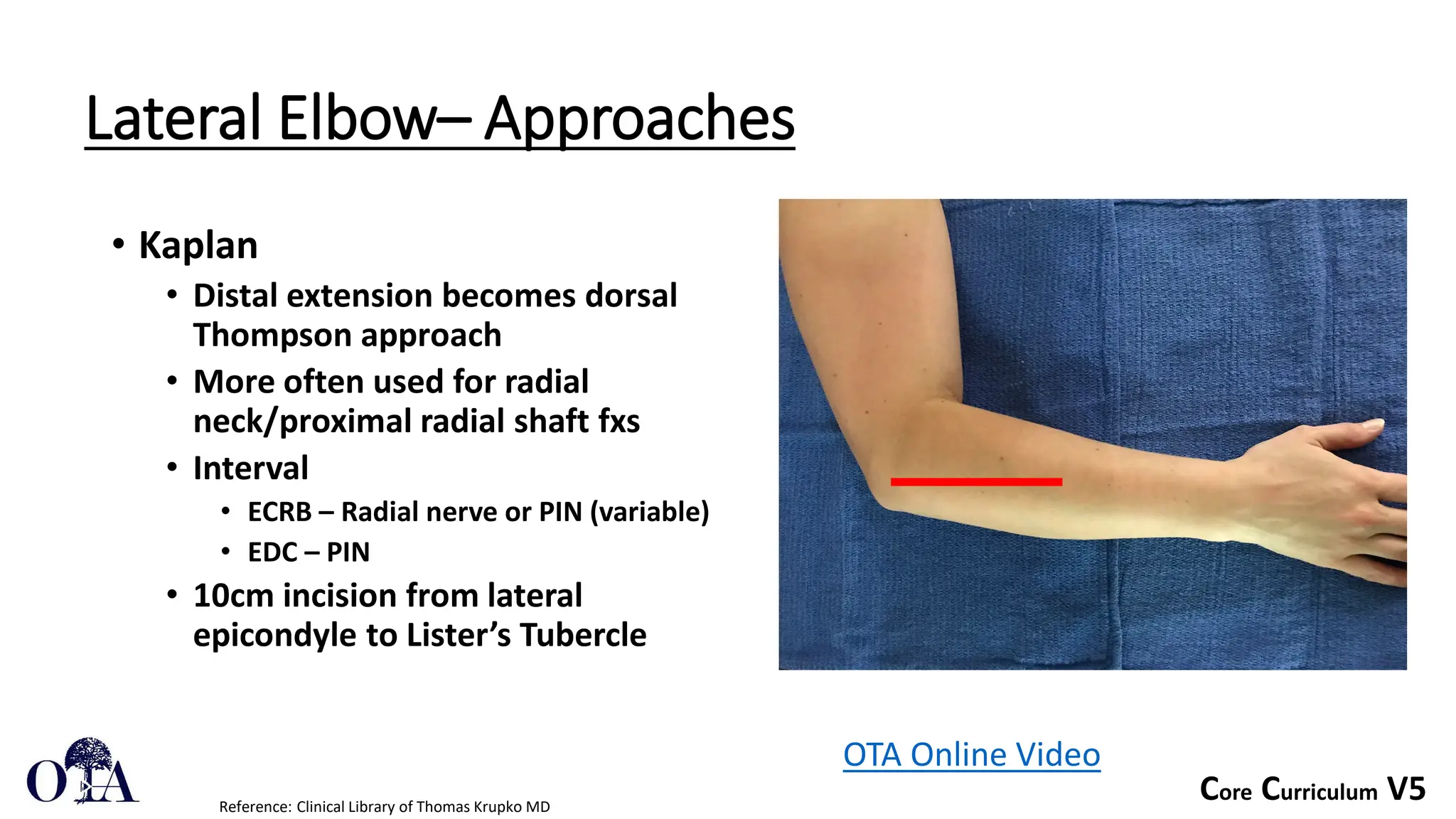
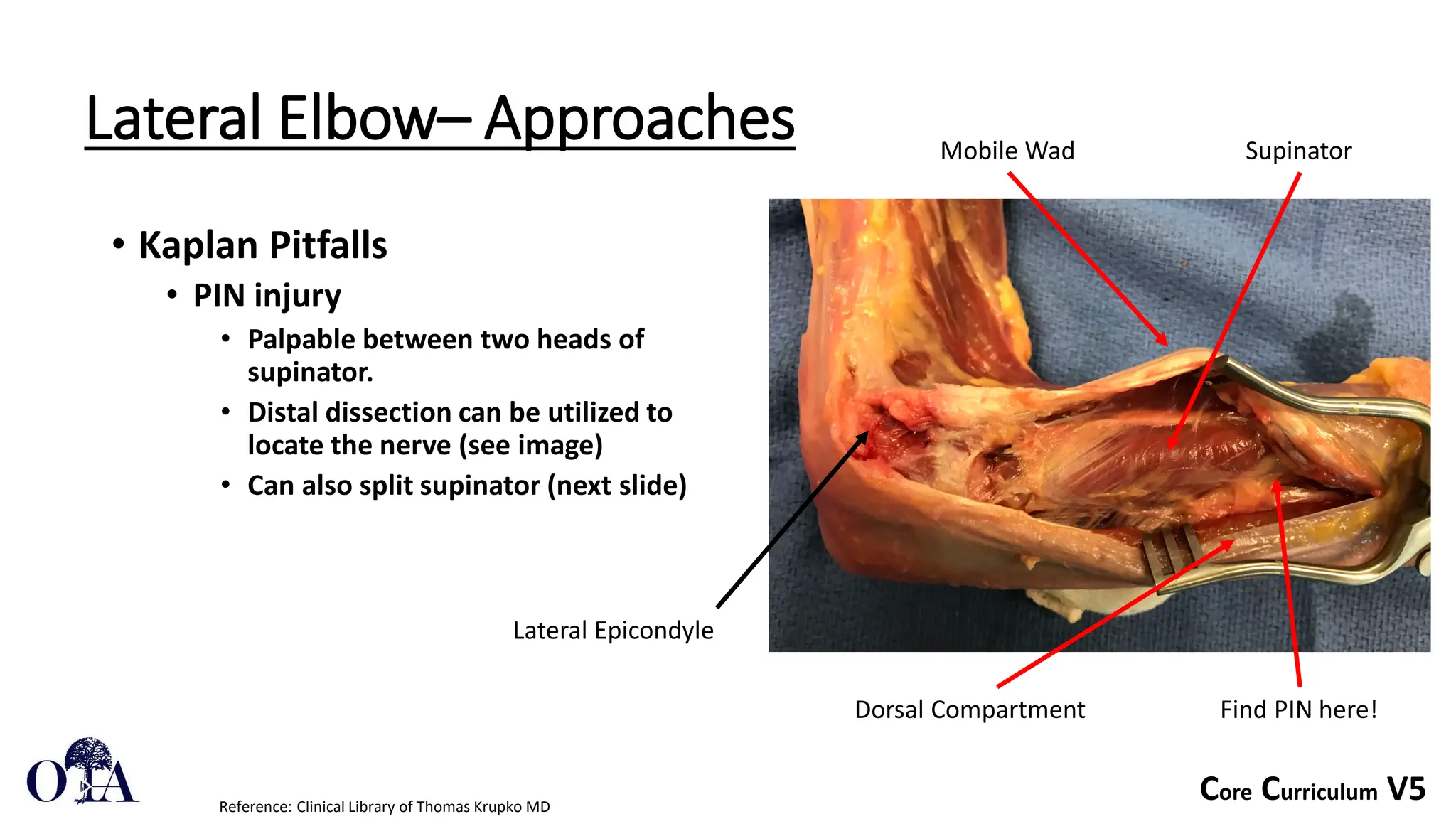
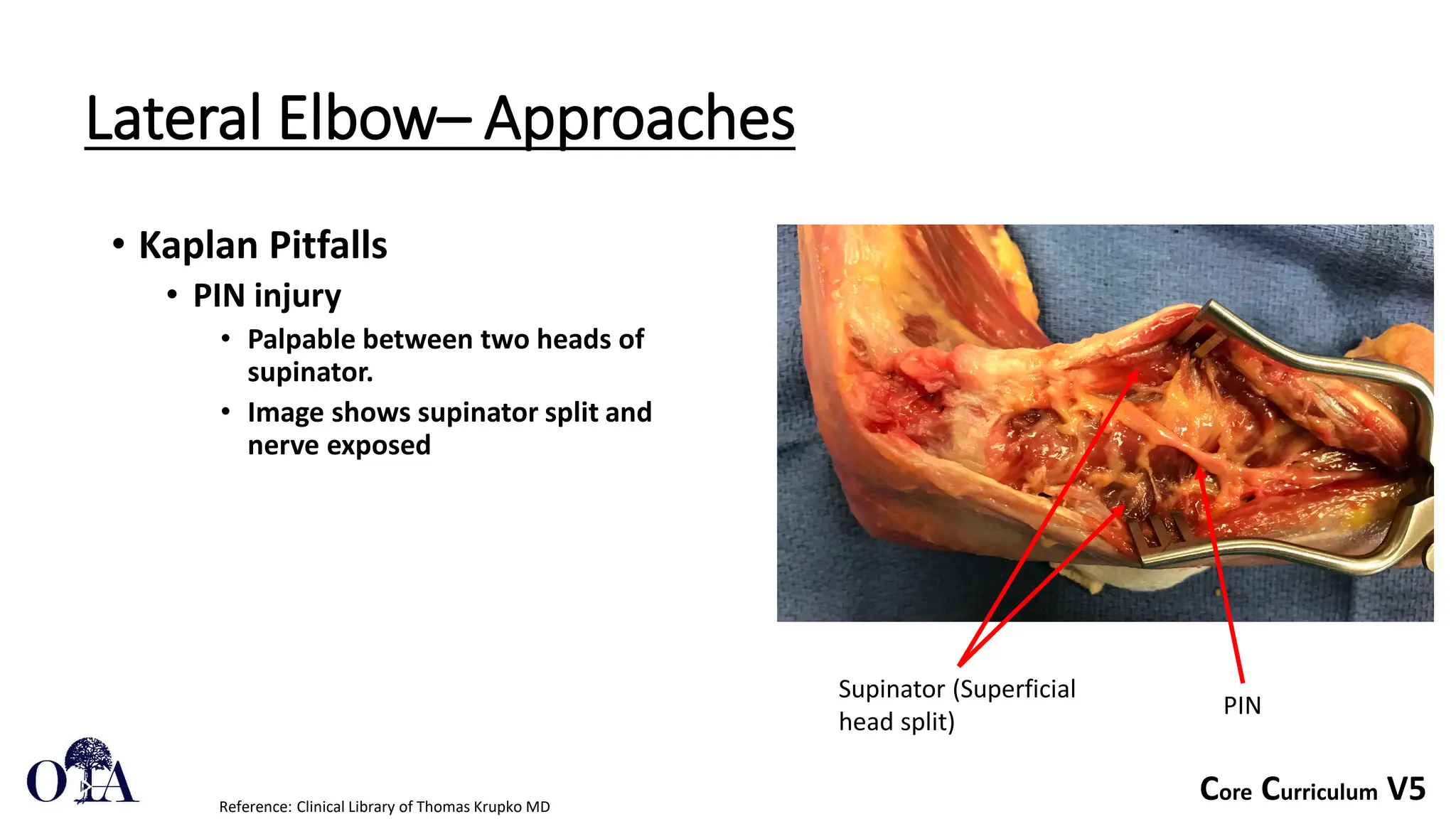
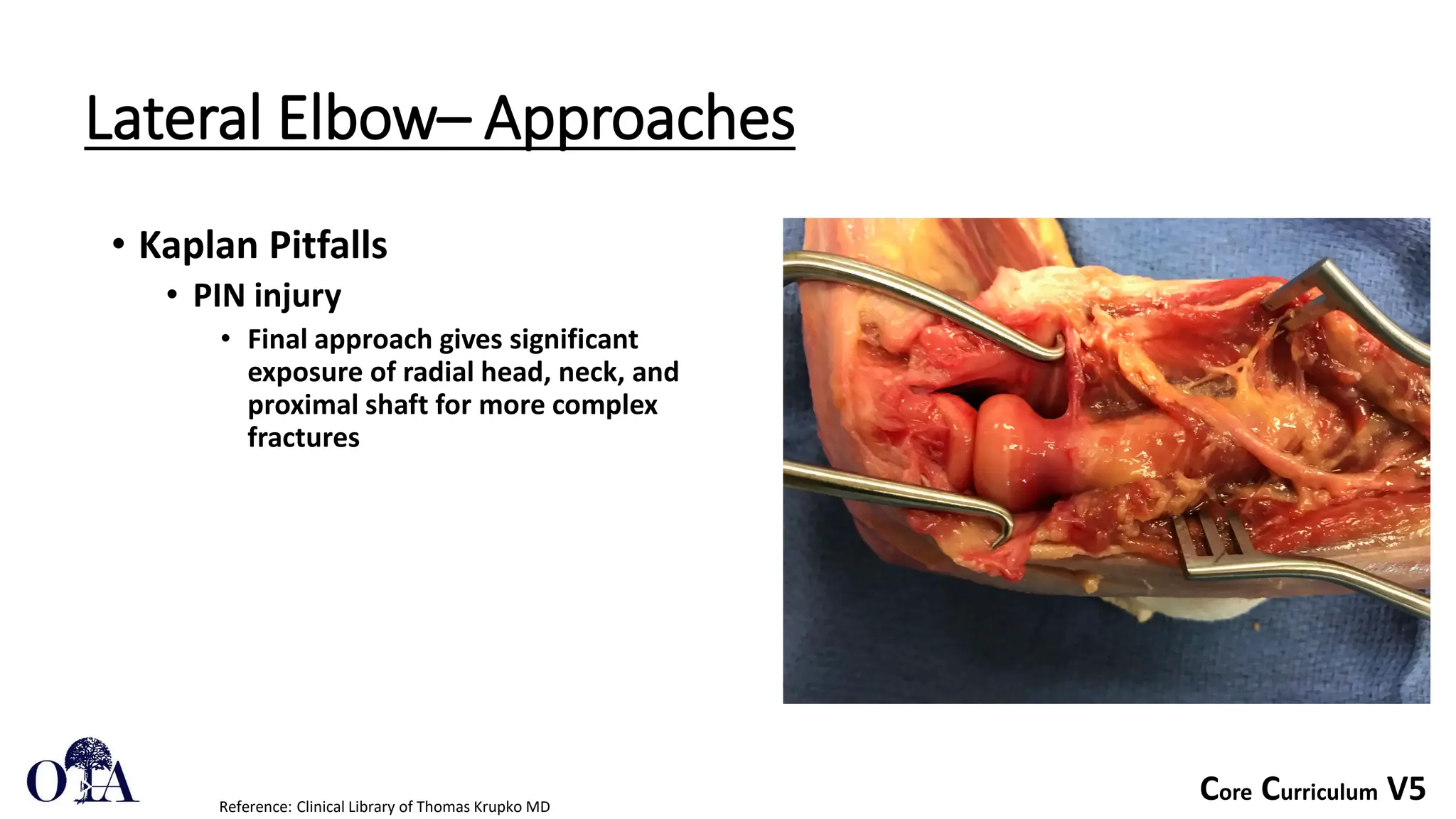
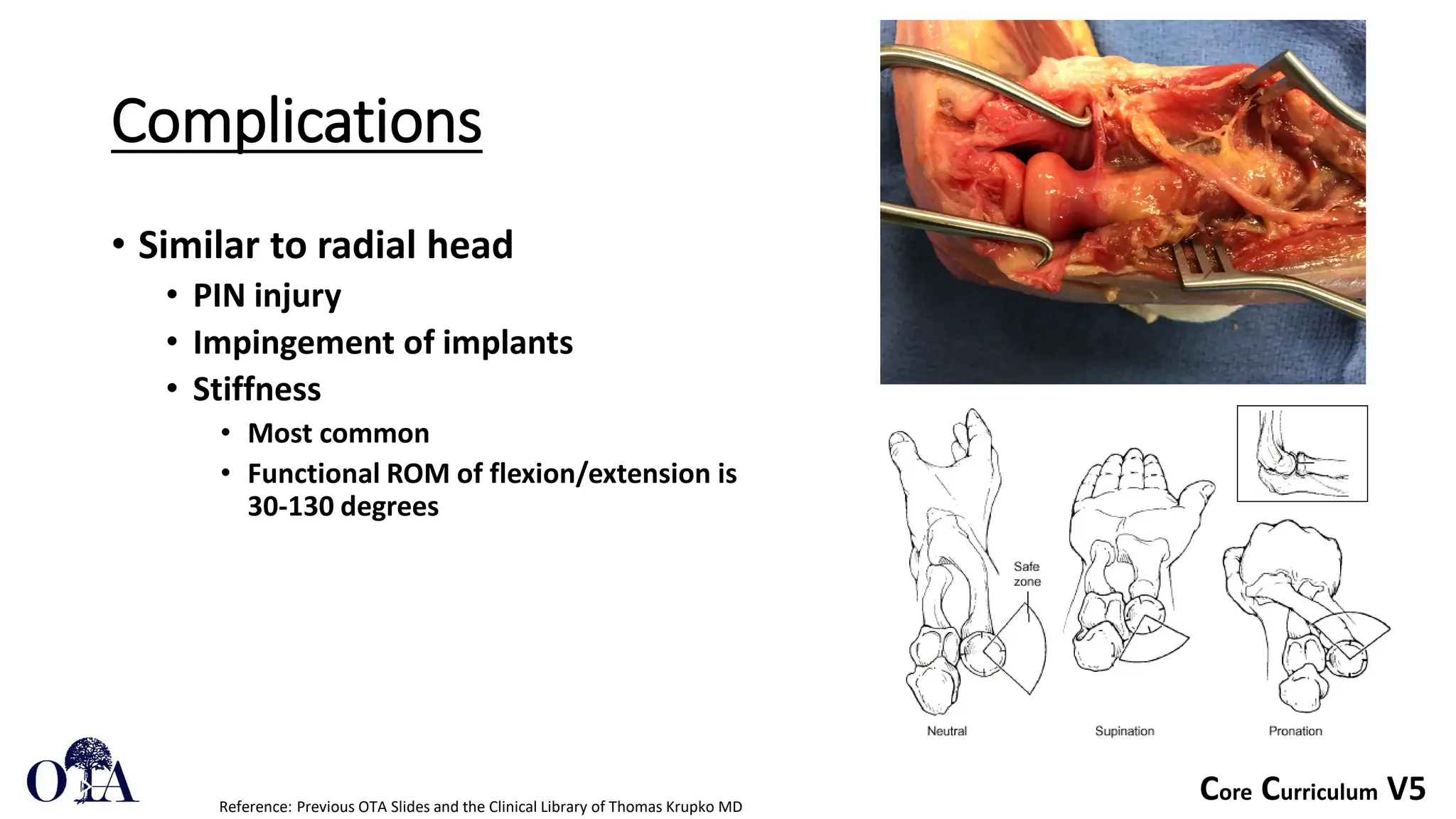
- Common approaches to the lateral elbow are the Kocher and Kaplan, which require care to avoid injury