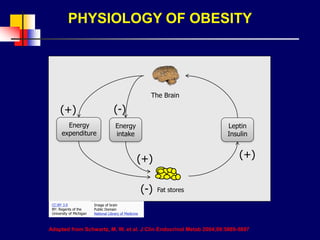
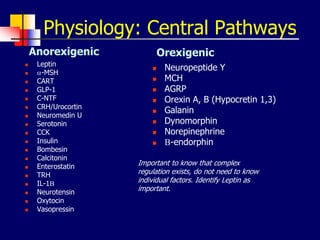
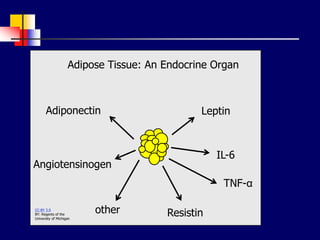
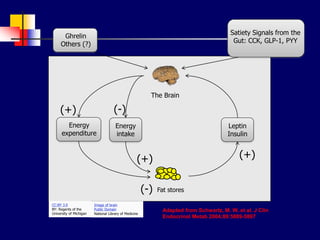
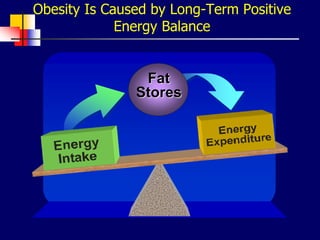
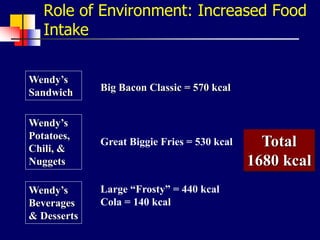
This document provides an overview and update on obesity. It begins by defining obesity based on BMI and body fat distribution. The physiology of obesity and factors regulating energy balance like leptin are described. Environmental and genetic causes of positive energy balance leading to obesity are discussed. Various endocrine conditions that can cause obesity are listed. The medical risks of obesity and approaches to treatment including prevention, diet, exercise, drugs, and surgery are summarized.