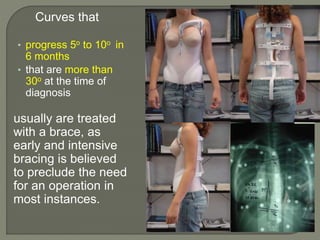
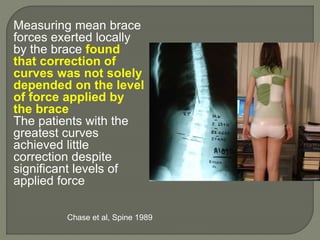
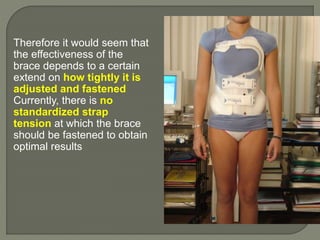
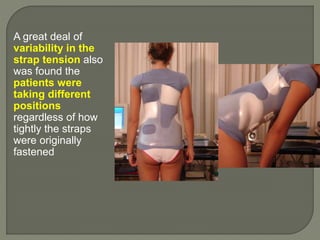
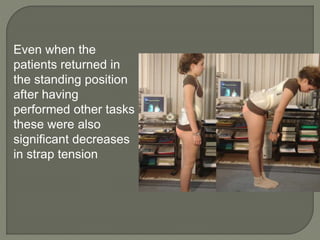
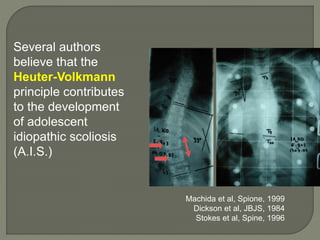
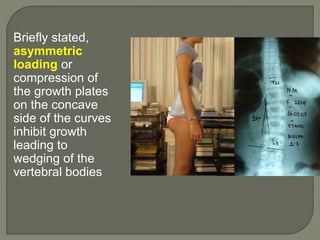
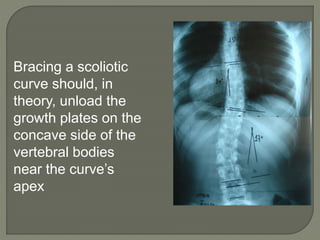
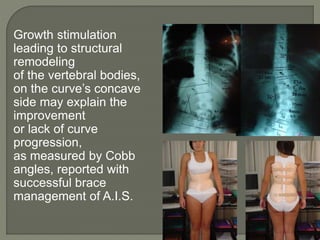
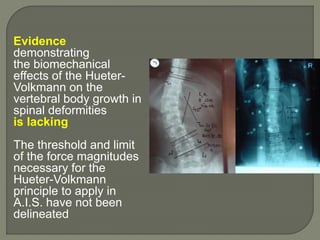
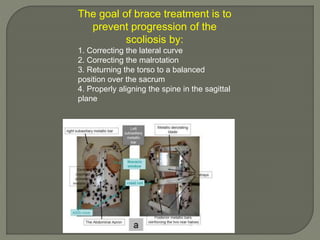
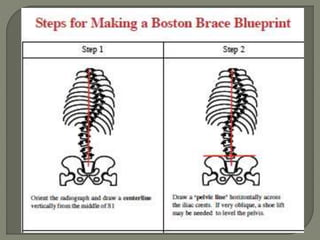
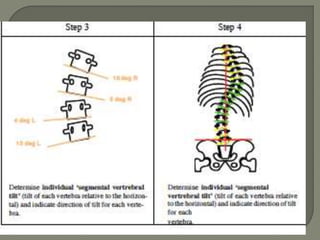
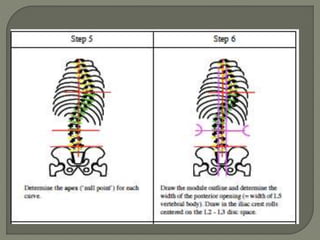
The document discusses the progression and treatment of scoliosis, particularly focusing on the effectiveness of brace treatments in managing curvature of the spine. It highlights the importance of curve magnitude at detection, the role of brace design and tension, and biomechanical principles such as the Hueter-Volkmann principle in guiding treatment outcomes. Evidence suggests that high strap forces and proper brace adjustments can significantly impact the success of non-operative interventions in idiopathic scoliosis.