Downloaded 363 times
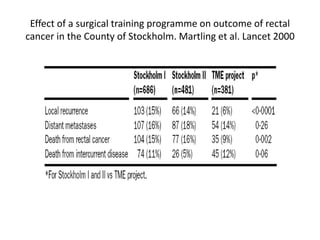
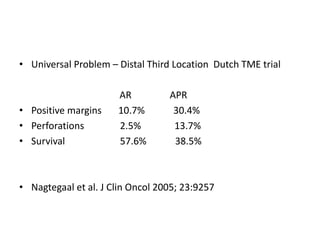
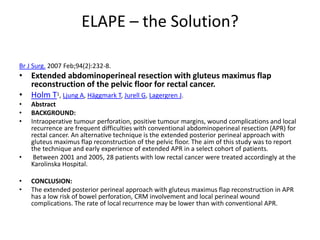
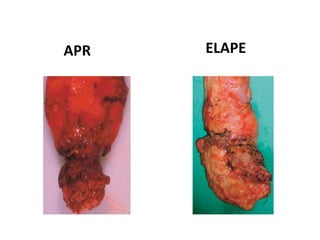




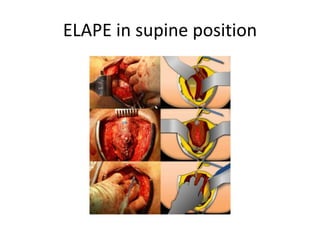

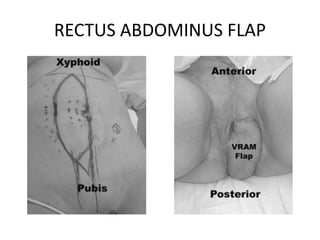

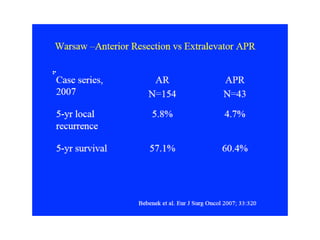
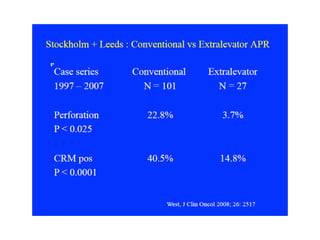
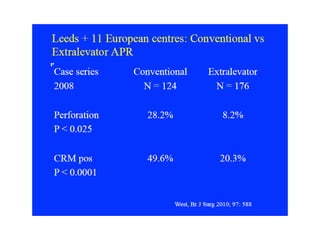
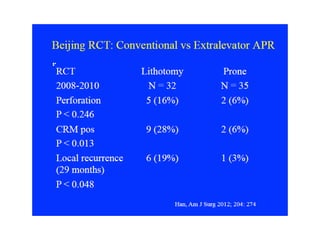
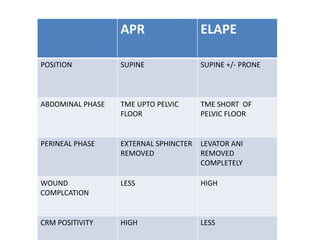

This document discusses the history and technique of the extended abdominoperineal excision (ELAPE) surgery for rectal cancer. It begins with Miles' description of the standard abdominoperineal resection (APR) in 1908. The ELAPE technique was developed to address high circumferential resection margin positivity and local recurrence rates with APR for low rectal cancers. The ELAPE surgery extends the abdominal phase of resection using total mesorectal excision principles and removes the levator muscles en bloc during the perineal phase. Initial studies show ELAPE reduces bowel perforation and positive margin rates compared to APR, with potentially lower local recurrence. However, large randomized controlled trials are still needed to establish EL

























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






