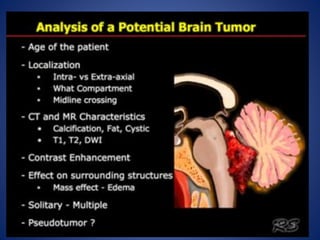
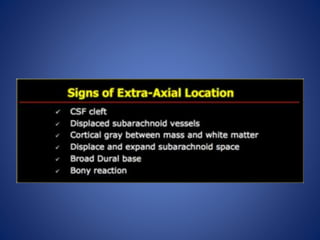
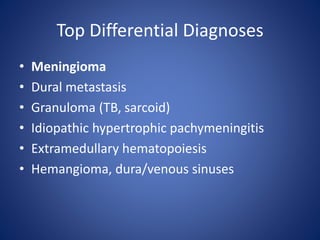
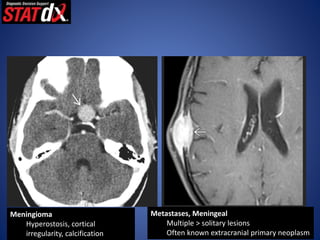
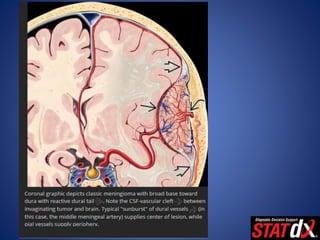
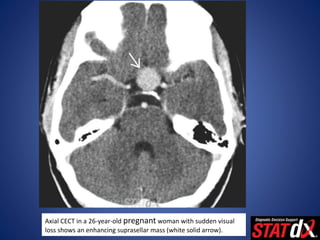
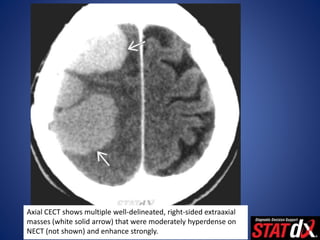
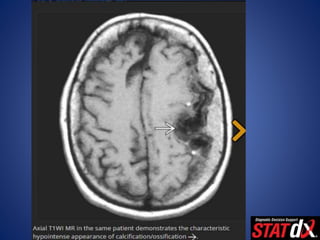
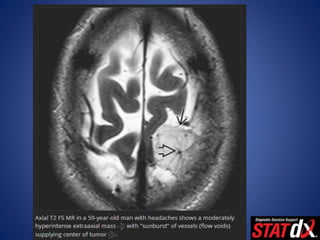
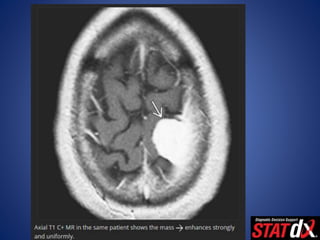
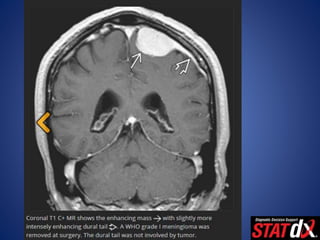
This document discusses extra-axial masses, specifically meningiomas. It provides details on the typical presentation, demographics, pathology, imaging features and diagnosis of meningiomas. On imaging, meningiomas usually appear as well-circumscribed, dural-based masses that enhance strongly with CT and MRI. They typically show calcification on CT and homogenous enhancement post-contrast. The document emphasizes that meningiomas are the most common extra-axial brain tumors and often appear as convexity or parasagittal masses, with females being more commonly affected.