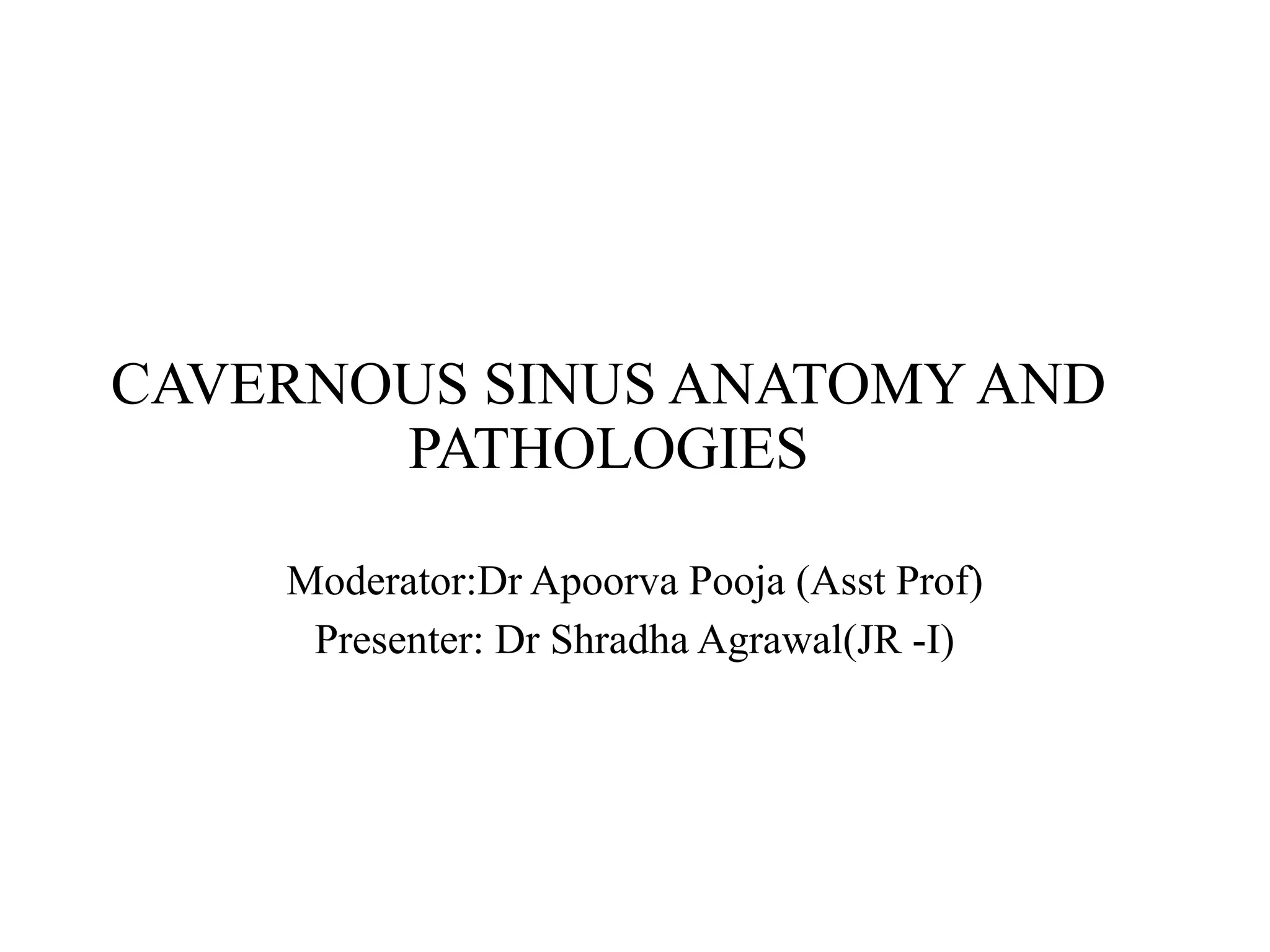
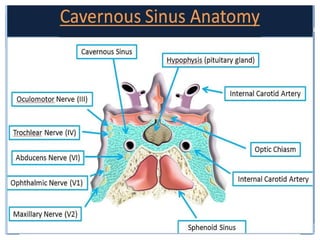
Cavernous Sinus Anatomy
Pairedcollection of thin walled veins between the endosteal and
meningeal dural layers located at the center of the head which
drains intracranial blood.
Anterior Border = Superior orbital fissure
Posterior Border = Petroclinoid fold and Clivus dura matter
Inferolateral Border =Inner middle cranial fossa
Lateral Border = Outer dural meningeal layer with deeper inner
nerve containing layer
Medial Border =Sella turcica.
4.
Venous Flow
Receives venoustributaries from the superior and inferior ophthalmic
veins and superficial cortical veins
Drains into the superior and inferior petrosal
sinuses
Connected to the venous basilar plexus posteriorly
• Nerves
–Lateral wall, superior to inferior
• CN III: Occulomotor nerve
• CN IV: Trochlear nerve
• CN V1: Ophthalmic nerve, the
V1 branch of the trigeminal
nerve
• CN V2: Maxillary nerve, the
V2 branch of CN V
– Paralleling internal carotid
artery
• CN VI: Abducents nerve
• Artery
– Internal carotid artery
Bends as the cavernous, C4
segment
– Bifurcates
Meningohypophysel trunk &
Inferolateral trunk
6.
Aneurysms
The diagnosis ofaneurysms is critically important in a sellar region
evaluation.
The arteries in the Willis´ polygon, which surrounds the sella turcica, are
the most frequent locations of intracranial aneurysms.
A round lesion with an internal signal void on spin echo MRI, especially
on those acquired with T2WI is a classic feature of an aneurysm with
rapid internal blood flow.
However, partially thrombosed aneurysms appear as well demarcated
round parasellar or intra-sellar lesions with internal T1WI hyperintensity
and characteristic heterogeneous T2WI hypointensity, findings that
indicate intra-aneurysmal clotting.
7.
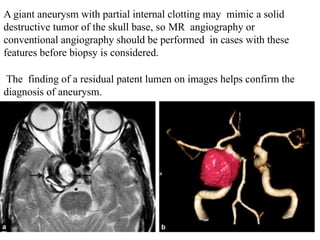
A giant aneurysmwith partial internal clotting may mimic a solid
destructive tumor of the skull base, so MR angiography or
conventional angiography should be performed in cases with these
features before biopsy is considered.
The finding of a residual patent lumen on images helps confirm the
diagnosis of aneurysm.
11.
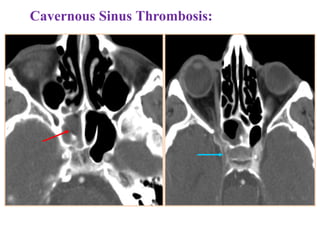
Cavernous sinus thrombosis:
It is a rare condition, most commonly infectious in nature, and the
diagnosis on imaging is not always straightforward.
It has high mortality and morbidity rates.
Orbital signs can include:
•chemosis/periorbital swelling
•Exophthalmos
Radiographic features
Cavernous sinus thrombosis is a clinical diagnosis.
12.
MRI with contrastis the imaging modality of choice to confirm its
presence and to differentiate it from alternatives such as
orbital cellulitis, which may have a similar clinical presentation.
CT
•non-contrast: high-density thrombus in affected cavernous sinus (seen
in only 25%)
•contrast-enhanced: distended cavernous sinus with a non-fat density
filling defect
MRI
•T1 and T2
• absent flow void
• signal characteristics vary depending on the age of the thrombus
but will be abnormal
•contrast-enhancement or lack of is not a reliable indicator as
organising thrombus can enhance
•diagnosis can generally be made on MR venography
13.
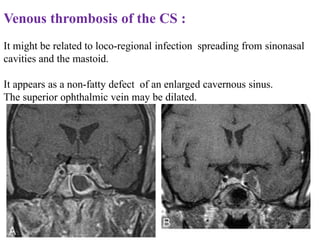
Venous thrombosis ofthe CS :
It might be related to loco-regional infection spreading from sinonasal
cavities and the mastoid.
It appears as a non-fatty defect of an enlarged cavernous sinus.
The superior ophthalmic vein may be dilated.
Carotid-cavernous fistula (CCF)
CCFis a traumatic or spontaneous abnormal communication between
the cavernous sinus and the ICA or the meningeal arterial branches of
the CS.
CCF can be a direct communication between cavernous ICA and the
cavernous sinus and is almost always caused by a traumatism or less
frequently by a ruptured ICA aneurysm.
Indirect CCF are dural shunts between the CS and the meningeal
branches of the cavernous ICA and/or external carotid artery.
17.
Radiographic features
CT
CT angiographyis the non-invasive imaging modality of choice for
evaluation of suspected caroticocavernous fistula .
Features include
•orbital congestion
• proptosis/exophthalmos
• retrobulbar fat stranding/oedema
• enlargement of extraocular muscles
•venous engorgement and enhancement
•enlarged superior ophthalmic vein
•bulging cavernous sinus
•asymmetric enhancement of cavernous sinus with attenuation similar
to that of internal carotid artery and higher than that of
transverse sinus
18.
•dehiscent internal carotidartery (for direct type fistulas): snowman
appearance of fistula tract involving the feeding carotid artery and
draining venous pouch
•intracranial haemorrhage from a ruptured cortical vein
Angiography (DSA)
Catheter-based digital subtraction angiography is the gold standard
imaging technique due to its superior spatial and temporal resolution.
•rapid shunting from internal carotid artery to cavernous sinus
•enlarged draining veins
•retrograde flow from cavernous sinus, most commonly into the
ophthalmic veins
Ultrasound
Doppler assessment may show arterialised enlarged ophthalmic veins.
Tolosa Hunt syndrome(THS)
THS is a non-specific granulomatous inflammation located in the
orbital apex and extending to the cavernous sinus.
THS can be bilateral in 5% of the patients.
It responds strongly to systemic corticosteroid.
It appears as a soft tissue mass, isointense to gray matter on T1-wi.
shows a variable signal on T2-wi and moderate to intense contrast
enhancement.
The cavernous ICA can be narrowed by the inflammatory process.
22.
Radiographic features
CT
May showasymmetrical enlargement in the region of the cavernous
sinus on the affected side +/- contrast enhancement .
The secondary criteria are internal carotid artery narrowing, extension
towards the superior orbital fissure and orbital apex.
MRI
May show evidence of inflammatory changes in the region of the
anterior cavernous sinus, superior orbital fissure +/- orbital apex. Signal
characteristics are non-specific (clinical scenario essential to diagnosis)
but may include:
•T1: involved region is isointense to hyperintense compared with
muscle
•T2: involved area is hyperintense
•T1 C+ (Gd): may show contrast enhancement during active phase with
resolution of enhancement following treatment ,
25.
Cavernous Sinus Tumors
Mostcommon etiology of cavernous sinus syndrome
Primary tumors
Schwannoma
Neurofibroma
Meningioma
Hemangioma
Lymphoma
Secondary involvement/Metastatic disease
Pituitary Adenoma
Nasopharyngeal carcinoma
Perineural spread of tumor through neural foramina Base of skull
tumor
Chondrosarcoma
Osteosarcoma
26.
Pituitary adenoma
Six to10% of pituitary adenomas invade the cavernous sinus,and
represents its most frequent lesion.
It is an intrasellar process with lateral extension to the cavernous sinus, in
opposition to other diseases originating from the CS.
These invasive pituitary adenomas are associated with more surgical
mortality and morbidity.
Macroadenomas (>1 cm) appear hypointense on T1- weighted image
(WI) and hyperintense on T2-wi. They enhance after gadolinium
administration, but less than normal pituitary tissue.
Invasion of the cavernous sinus is secondary to the perforation of its
medial wall, and is very likely if the lateral intercarotid line is crossed or
if the encasement of the intracavernous ICA by the tumor is greater than
or equal to 67%.
27.
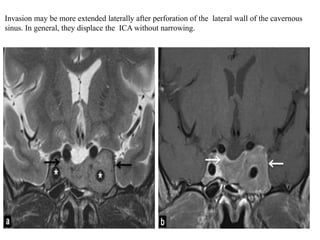
Invasion may bemore extended laterally after perforation of the lateral wall of the cavernous
sinus. In general, they displace the ICA without narrowing.
29.
Meningioma.
Meningiomas became upto 18% of all intracranial tumors.
They may arise from a suprasellar or parasellar location.
Suprasellar meningiomas commonly arise from the diaphragm sellae or
tuberculum sellae, and vision defects caused by compression of the optic
chiasm are common clinical findings.
Large meningiomas originating along the planum sphenoidale or greater
wing of the sphenoid bone may extend into the suprasellar cistern or
parasellar regions.
These tumors may be entirely parasellar if they originate from the dural
wall of the cavernous sinus. Meningiomas are generally isointense
relative to cortical gray matter on T1- and T2- weighted images.
32.
Schwannoma:
They are lesscommonly called neurinomas or neurilemmomas, are
benign tumours of Schwann cell origin and are the most common
tumour of peripheral nerves, including cranial nerves.
They may grow primarily in the parasellar region or extend posteriorly
through the porus trigeminus into the posterior fossa.
Tumor extension into the pterygoid fossa or paranasal sinuses occurs in
10% of cases.
The pressure exerted by the tumor leads to erosion of the underlying
bone and enlargement of the foramen ovale, foramen rotundum, or the
superior orbital fissure, which is better appreciated on thin-section
coronal-CT scans.
33.
Trigeminal schwannomas typicallyfollow the course of the fifth
cranial nerve and have a dumbbell-shaped configuration.
They are smoothly marginated tumors and are usually isointense
comparing to gray matter on T1WI and hyperintense on T2WI.
Small tumors are homogeneous; large tumors can have heterogeneous
signal intensity due to degenerative changes, including cyst formation
and fatty degeneration.
General imaging featuresof schwannomas include:
•well-circumscribed masses which displace adjacent structures
without direct invasion.
•cystic and fatty degeneration is common.
•the larger a schwannoma, the more likely it is to show heterogeneity
because of cystic degeneration or haemorrhage.
•haemorrhage occurs in 5% of cases..
•calcification is rare
37.
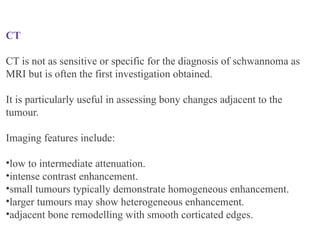
CT
CT is notas sensitive or specific for the diagnosis of schwannoma as
MRI but is often the first investigation obtained.
It is particularly useful in assessing bony changes adjacent to the
tumour.
Imaging features include:
•low to intermediate attenuation.
•intense contrast enhancement.
•small tumours typically demonstrate homogeneous enhancement.
•larger tumours may show heterogeneous enhancement.
•adjacent bone remodelling with smooth corticated edges.
38.
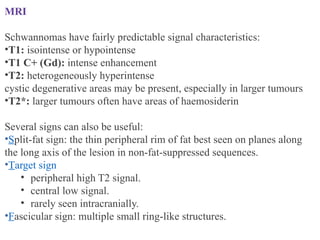
MRI
Schwannomas have fairlypredictable signal characteristics:
•T1: isointense or hypointense
•T1 C+ (Gd): intense enhancement
•T2: heterogeneously hyperintense
cystic degenerative areas may be present, especially in larger tumours
•T2*: larger tumours often have areas of haemosiderin
Several signs can also be useful:
•Split-fat sign: the thin peripheral rim of fat best seen on planes along
the long axis of the lesion in non-fat-suppressed sequences.
•Target sign
• peripheral high T2 signal.
• central low signal.
• rarely seen intracranially.
•Fascicular sign: multiple small ring-like structures.
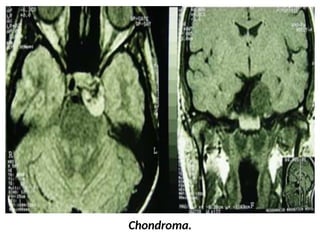
Chordoma and Chondrosarcoma
Chondromatoustumors develop from embryonic cartilaginous remnants
enclosed in the bones of the skull base.
They often arise from the petrooccipital or sphenooccipital
synchondrosis and destroy the adjacent bones.
Chondromatous tumors can be hypoattenuating at CT, possibly with a
marginal high- attenuation area due to a dense matrix of hyaline
cartilage or massive calcification. Lytic bone erosion may be seen.
At MR imaging, the tumor is hypointense on T1- weighted images and
heterogeneously hyperintense on T2-weighted images; it enhances
poorly due to its hypovascularity.
Hemangioma
It's a vascularlesion rarely located in the CS. Differential diagnoses
include meningioma and schwannoma.
Hemangioma appears isodense or slightly hyperdense compared with
surrounding structures on CT, and does not contain calcifications.
The characteristic imaging findings are a high signal in T2-wi and a
progressive and strong centripetal enhancement.
47.
Nasopharyngeal carcinoma:
It caninvolve the CS by direct skull base invasion, through the foramen
lacerum, or along the branches V2 and V3 of trigeminal nerve.
The tumor appears hypointense on T2-wi, hypo- to isointense on T1-wi
and enhances after contrast.
The perineural spread is depicted by an enlarged and enhanced nerve
associated with an enlargement of its foramina
49.
Epidermoid cyst
CS epidermoidcysts are rare and can involve it in three different
ways; an extracavernous epidermoid cyst can invade and compress
the CS.
It can arise from the lateral dural wall of the CS. Finally, it can be
located inside the CS.
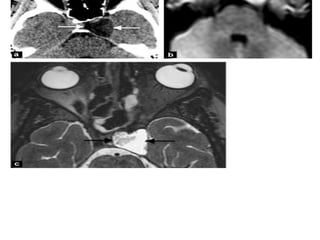
They appear hypodense on CT. The main features are a
heterogeneous hyper signal on FLAIR and high resolution T2
imaging, and high signal intensity on diffusion WI. They show no
enhancement .
#7 Aneurysm: axial T2-wi (a) shows a heterogeneous and enlarged right cavernous sinus with a multilayer appearance (black arrows) corresponding to a giant intracavernous aneurysm. Note the mass effect on the right temporal lobe.
See also the 3D volume rendering showing the aneurysm (b).
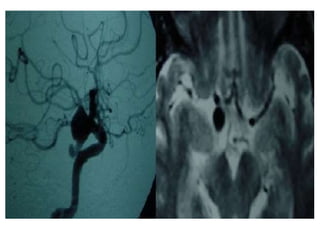
#9 Right posterior communicating artery aneurysm digital angiography and MR.
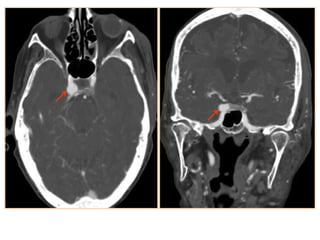
#10 Intracavernous aneurysms. A, Axial T2-weighted image shows a left intracavernous ICA (A) aneurysm. Note flow artifacts (arrow) confirming the pulsatile nature of the lesions. B, Coronal postcontrast maximum-intensity image from a CT angiogram in the same patient shows the left intracavernous aneurysm.
#12 Differential diagnosis
Consideration is given to other causes of cavernous sinus syndrome and painful ophthalmoplegia caused by local compression of which 30% are tumours 7:
carotid-cavernous fistula
superior orbital fissure syndrome
meningioma
Tolosa-Hunt syndrome
lytic bone lesions
cavernous haemangioma
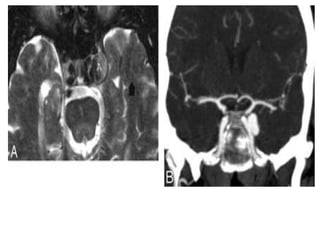
#13 CS thrombosis. A, Coronal post contrast T1-weighted image shows an enlarged and inhomogeneous-appearing right CS that contains areas of low signal intensity (arrow) compatible with clot. B, Coronal post contrast T1-weighted image in a different patient shows a large nonenhancing clot expanding the left CS. The ipsilateral ICA is slightly narrowed.
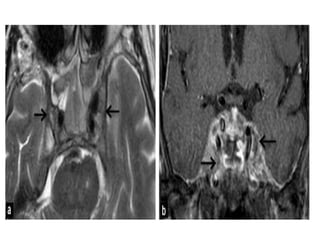
#14 Venous thrombosis: bilaterally heterogeneous and enlarged cavernous sinus on T2-wi (a), containing low signal areas on enhanced T1-wi suggesting clots (blacks arrows: b).
#15 Acute fulminant invasive mucormysosis with sphenoid sinusitis complicated by acute cavernous sinus thrombosis
#16 Direct-There are a number of causes, however, aneurysm rupture and trauma are by far the most common:
ruptured intracavernous carotid artery aneurysm
trauma (including surgery/angiography)
other causes include
collagen deficiency syndromes
fibromuscular dysplasia
arterial dissection
Indirect they are postulated to occur secondary to cavernous sinus thrombosis with revascularisation and thus are similar to dural arteriovenous fistulas elsewhere.
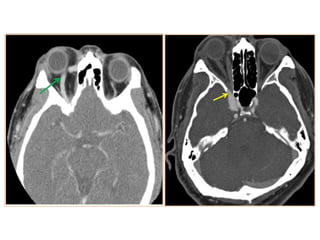
#19 Carotid-Cavernous (C-C) Fistula.
Enlarged right superior ophthalmic vein with early arterial enhancement of the right cavernous sinus suggestive of carotid cavernous fistula
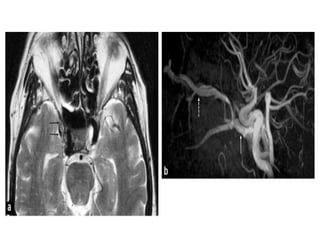
#20 Carotid-cavernous fistula: axial T2-wi (a) of a carotid-cavernous fistula appearing as a heterogeneous signal with flow voids of the right cavernous sinus (black arrows). Note the dilatation of the superior ophthalmic vein (dotted arrow) and the carotid-cavernous fistula (white arrow) on an arterial TOF of another patient with a carotid-cavernous fistula (b)
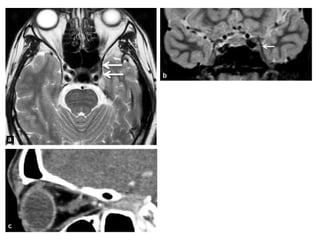
#23 Tolosa Hunt syndrome: axial (a) and coronal (b) T2-wi, sagittal
(c) enhanced CT, showing a insular hypointense enlargement of the left cavernous sinus (arrows) with an enhancement and an extension to the orbital apex (star on image c). These findings are consistent with a Tolosa Hunt syndrome.
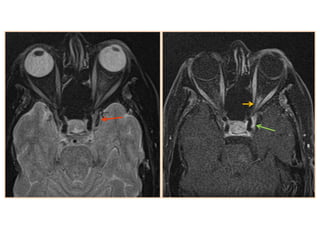
#24 Tolosa-Hunt SyndromeT2 iso-hypointense signal in the left cavernous sinus with enhancement
Enhancement is also seen in the left superior orbital fissure
#27 Pituitary adenoma. Coronal T2-wi (a) and coronal enhanced T1-wi (b) showing an enhancing pituitary adenoma (arrows), appearing hyperintense on T2-wi and invading the left cavernous sinus with an encasement of the left internal carotid artery. Note the displacement of the arteries by the mass (stars) without stenosis.
#28 Large enhancing pituitary mass extending to the right cavernous sinus and encasing the right ICA.
#30 Meningioma: axial T2-wi (a) and T1-wi after contrast (b) showing a left cavernous sinus mass (white arrows) slightly hypointense on T2 sequence with strong and homogeneous enhancement. This lesion presents a dural tail anteriorly and posteriorly and totally encases the intracavernous left internal carotid artery, which is narrowed (black arrow).
#31 T2 isointense left cavernous sinus meningioma with narrowing of the left ICA
#34
The differential varies according to the size of the lesion and the location. In most cases, where the lesion is large and extends both into the cerebellopontine angle, the differential includes:
vestibular schwannoma: ~80% of CPA masses
meningioma: ~10% of CPA masses
ependymoma
metastasis
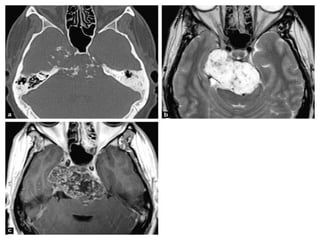
Chondrosarcoma
When small and confined to Meckel's cave the differential also includes:
ICA aneurysms and vascular malformations
pituitary macroadenoma
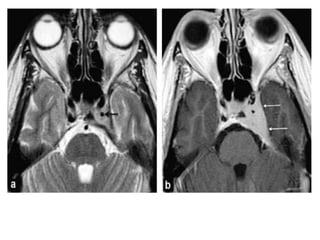
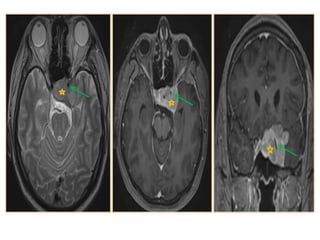
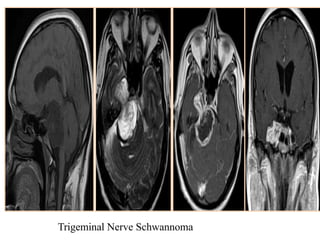
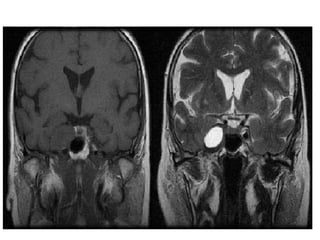
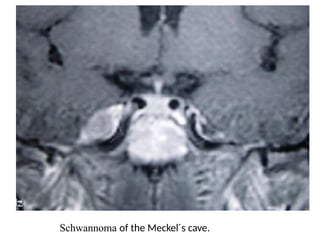
#35 Schwannoma of the trigeminal nerve (T1-weighted sequences and T2).
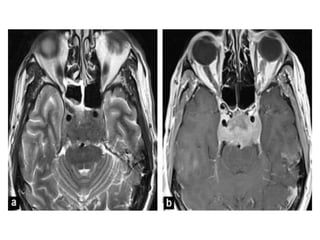
#41 Chondrosarcoma: large mass localized on the right petroclival fissure invading the right cavernous sinus and extending to the posterior fossa with mass effect on the pons.
CT shows stippled calcifications and petrous apex erosion (a).
This mass is strongly hyperintense on T2-wi (b),
and shows heterogeneous enhancement after contrast (c).
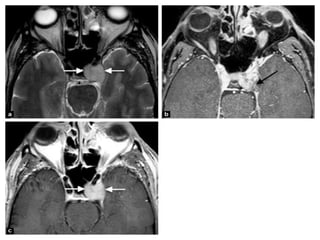
#42 Chordoma: mass centered on the clivus and the right cavernous sinus, heterogeneously hyperintense on T2-wi.
(a), hypo- to isointense on T1-wi with an heterogeneous enhancement after contrast
(b) corresponding to a chordoma.
#45 Cavernous hemangiomas.
A, Axial post contrast T1-weighted image shows a large and homogeneously enhancing mass arising from the lateral wall of the left CS.
B, Axial post contrast T1-weighted image in a different cavernoma, which shows inhomogeneous contrast enhancement but also arises from the lateral wall of the CS, pushing the ICA (arrow) medially. When a mass arises in the lateral wall of a CS, the most important differential diagnosis is that of meningioma versus cavernoma.
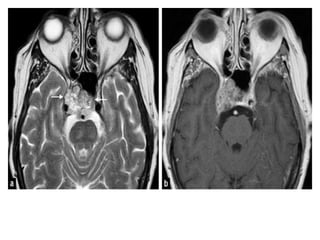
#46 Hemangioma: hemangioma appears as a very well delineated lesion of the left cavernous sinus (white arrows), hyperintense on T2-wi (a),
associated with progressive and centripetal enhancement (black arrow: b, c).
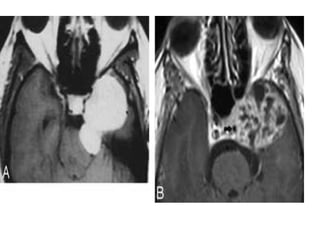
#48 Nasopharyngeal carcinoma: nasopharyngeal carcinoma invading both cavernous sinuses with carotid encasement and mass effect on
the pons.
The tumor appears with an intermediate signal on T2-WI (a)
and heterogeneous enhancement on T1-wi after contrast (b).