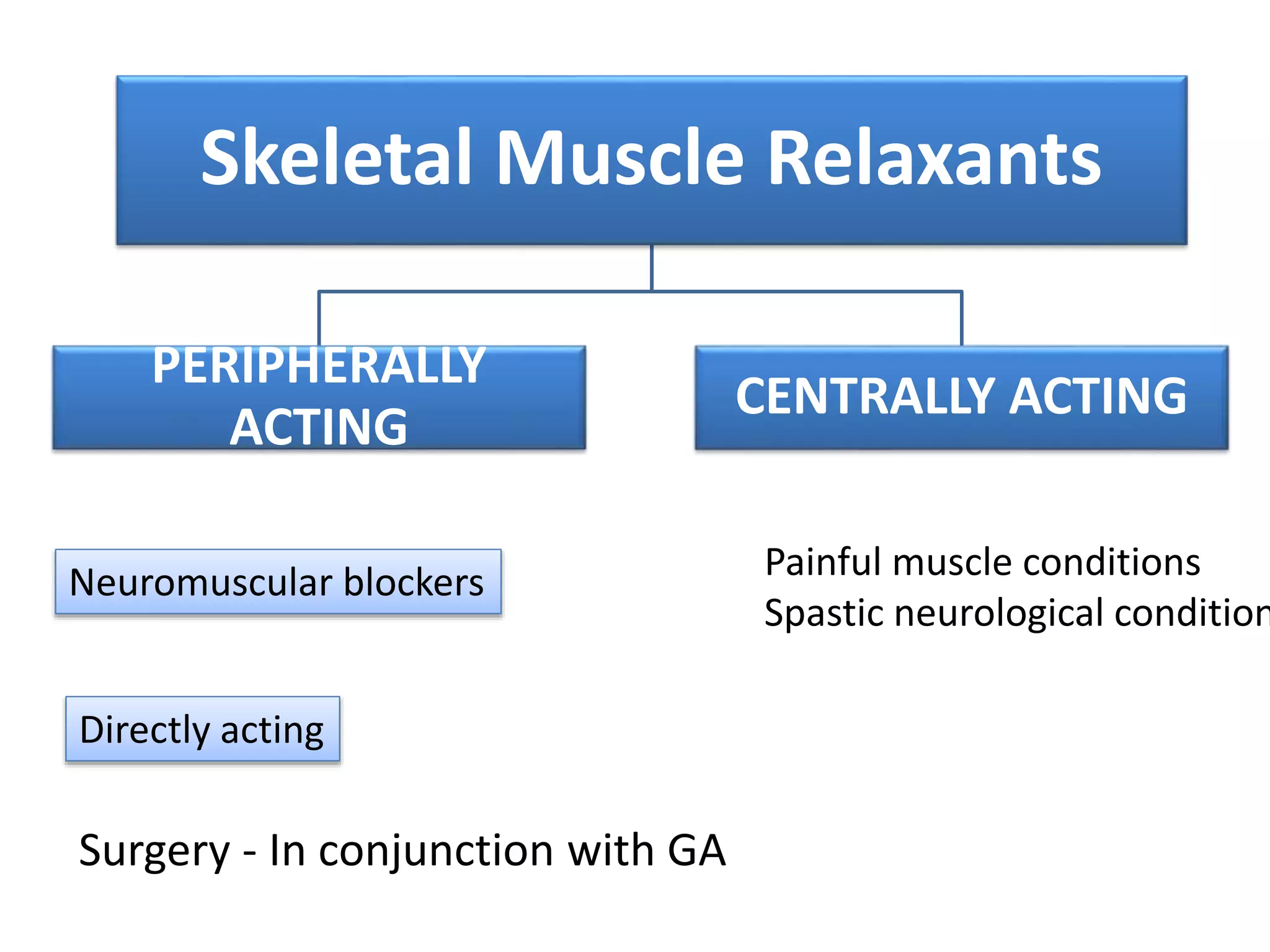
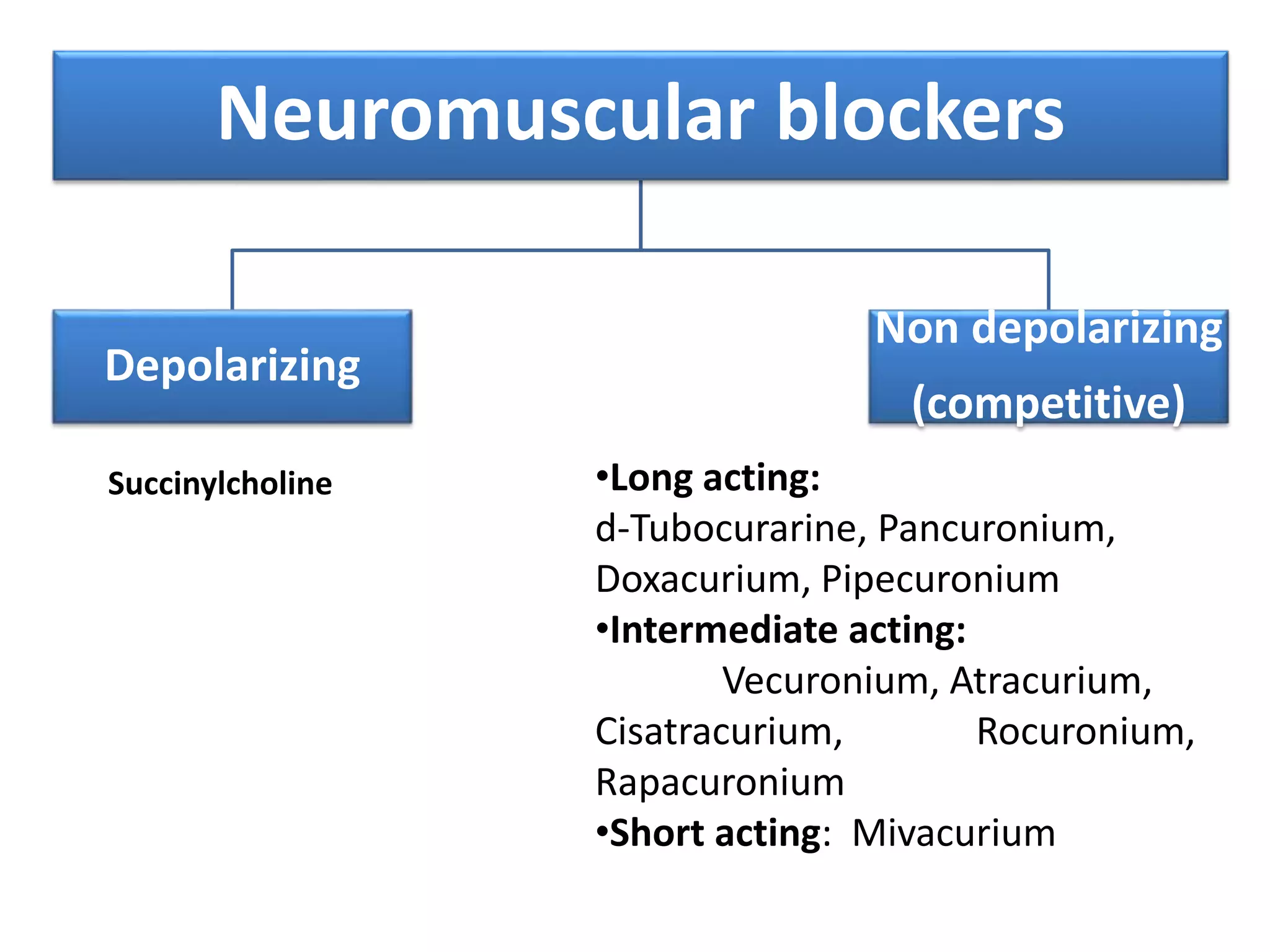
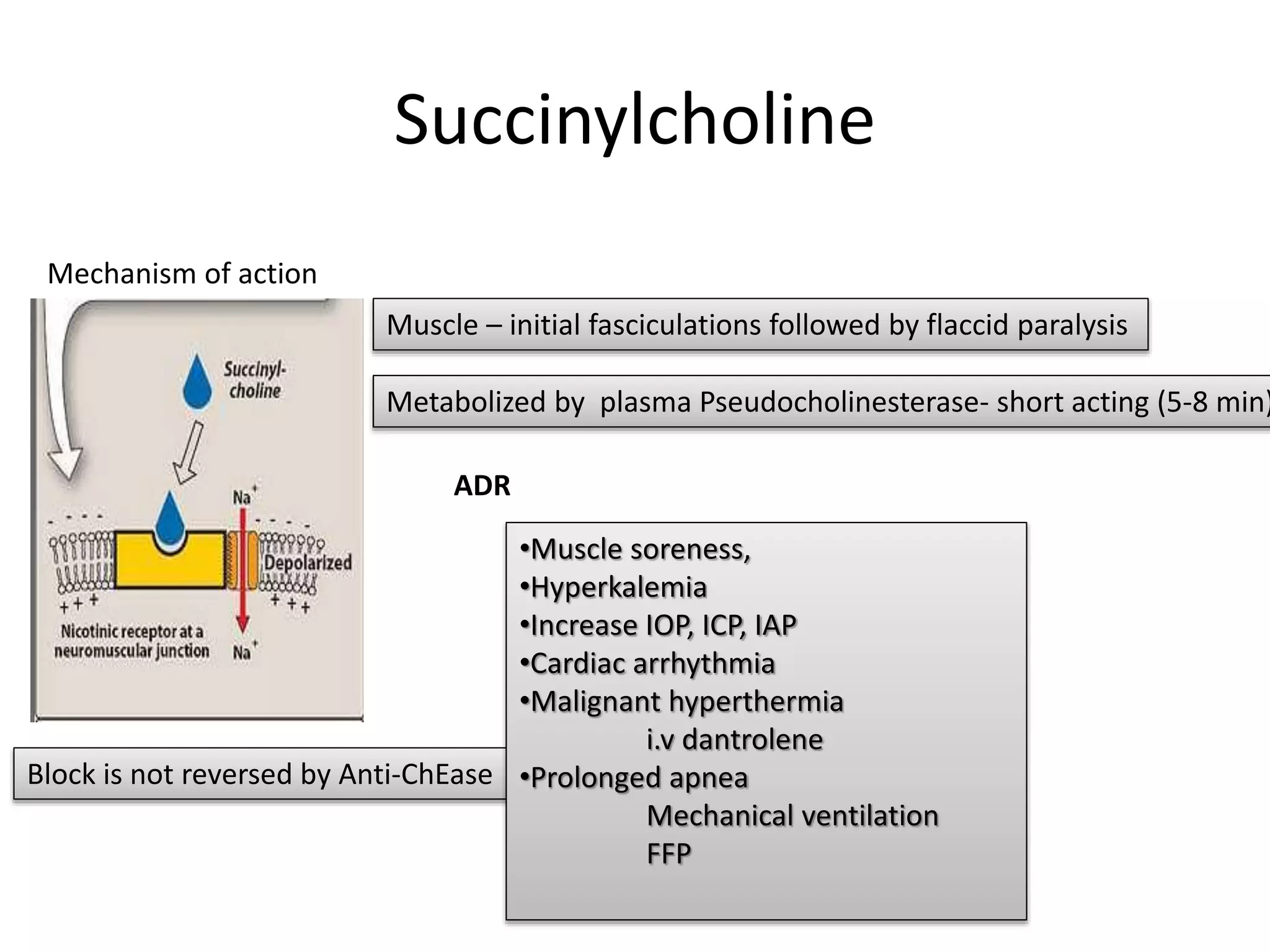
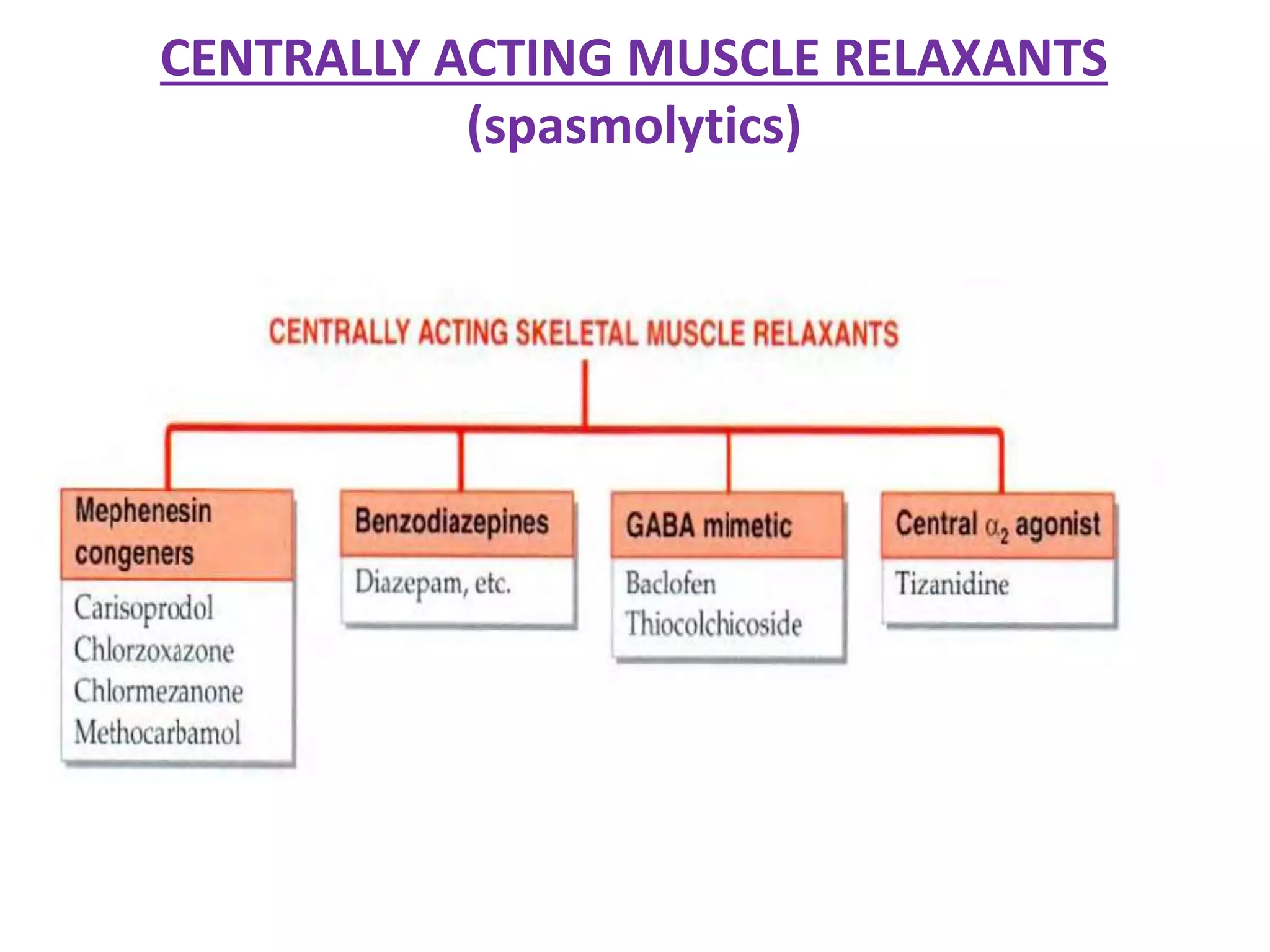
Skeletal muscle relaxants can be peripherally or centrally acting. Peripherally acting ones include neuromuscular blockers which can be depolarizing like succinylcholine or non-depolarizing like d-tubocurarine. They work by blocking neuromuscular transmission. Newer blockers have fewer side effects than older ones. They are used during surgery or mechanical ventilation. Centrally acting ones like dantrolene and baclofen work by reducing muscle tone. They are used for spasticity, spasms, and spastic neurological diseases.