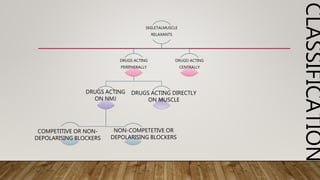
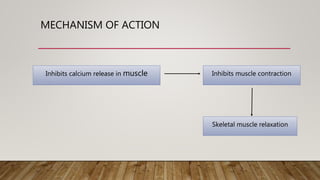
The document discusses skeletal muscle relaxants, which are categorized into neuromuscular blockers and spasmolytics, detailing their mechanisms, pharmacological actions, and classifications. It describes peripheral acting muscle relaxants that block neuromuscular junctions and central acting muscle relaxants that act on higher centres, highlighting their uses in various medical procedures and spastic disorders. Additionally, it covers adverse effects, treatment of toxicity, pharmacokinetics, and nursing implications for patients using these drugs.