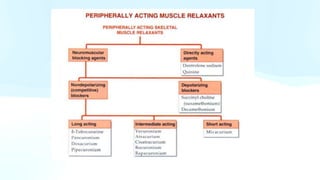
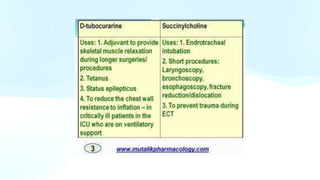
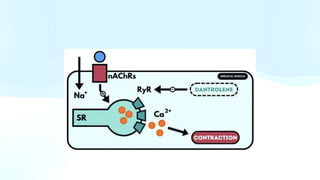
The document discusses skeletal muscle relaxants, which can be categorized into peripherally and centrally acting types. Peripherally acting agents, such as succinylcholine, are used for procedures requiring muscle relaxation, while centrally acting relaxants are primarily used for conditions like cerebral palsy and trauma. Dantrolene is highlighted as a directly acting muscle relaxant for treating malignant hyperthermia, and botulinum toxin A is mentioned for its role in treating muscle spasticity and cosmetic applications.