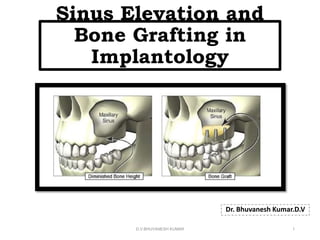
The document discusses sinus elevation and bone grafting procedures for dental implant placement. It begins with an overview of the anatomy of the maxillary sinus and classifications for the amount and density of available bone. It then covers indications such as pneumatization of the sinus and contraindications like uncontrolled sinusitis. The document reviews sources of graft materials, including autografts obtained from intraoral and extraoral donor sites. Techniques for sinus elevation via lateral wall approach or osteotome are presented along with case classifications and guidelines for surgical protocols.
Sinus lift Technique| Direct and Indirect Sinus Lift Technique| Dr. Rajat Sachdeva
Sinus Lift Technique
While placing Dental Implants on posterior region of upper jaw, due to either expansion of Maxillary Sinus as age advances or ridge resorption occurs because of various reason, dental implants cannot be placed on inadequate bone.
Sinus Lift procedure, to elevate Sinus Membrane through bone graft from socket, and Implant installation these indirectly augment the ridge and is called Indirect Technique.
And if it is done through Cald-well-luc procedure, it is called Direct Sinus Technique.
Learn more, follow our link:-
• Google+ link: g.page/delhidental/review
• Facebook link: https://goo.gl/tui98A
• Youtube link: https://goo.gl/mk7jfm
• Linkedin link: https://goo.gl/PrPgpB
• Slideshare link : http://goo.gl/0HY6ep
• Twitter Page : https://goo.gl/tohkcI
• Instagram page : https://goo.gl/OOGVig
Split ridge and expansion techniques are effective for the correction of moderately resorbed edentulous ridges in selected cases.
Transverse expansion is based on osseous plasticity obtained by corticotomy. It progressively allows for an adequate transversal intercortical diameter large enough to insert one or several dental implants.
The gap created by sagittal osteotomy expansion undergoes spontaneous ossification, following a mechanism similar to that occurring in fractures.
socket shield technique is a modified method of implant placement where many short comings of implant placement can be solved...
it is nothing but retaining of buccal cortical plate during extraction and implant is placed immediatly
The maxillary sinuses were first illustrated and described by Leonardo Da Vinci in 1489 and later documented by the English anatomist Nathaniel Highmore in 1651.
The maxillary sinus, or antrum of Highmore, lies within the body of the maxillary bone and is the largest and first to develop of the paranasal sinuses.
Shape- a pyramid-shaped cavity; base- adjacent to the nasal wall; apex- pointing to zygoma.
Size- insignificant until eruption of permanent dentition; average dimensions of adult sinus- 2.5–3.5 cm wide, 3.6–4.5 cm tall, and 3.8–4.5 cm deep; estimated volume of approximately 12–15 cm.
Extent- Anteriorly, extends to canine and premolar area. sinus floor usually has its most inferior point near the first molar region.
Sinus lift Technique| Direct and Indirect Sinus Lift Technique| Dr. Rajat Sachdeva
Sinus Lift Technique
While placing Dental Implants on posterior region of upper jaw, due to either expansion of Maxillary Sinus as age advances or ridge resorption occurs because of various reason, dental implants cannot be placed on inadequate bone.
Sinus Lift procedure, to elevate Sinus Membrane through bone graft from socket, and Implant installation these indirectly augment the ridge and is called Indirect Technique.
And if it is done through Cald-well-luc procedure, it is called Direct Sinus Technique.
Learn more, follow our link:-
• Google+ link: g.page/delhidental/review
• Facebook link: https://goo.gl/tui98A
• Youtube link: https://goo.gl/mk7jfm
• Linkedin link: https://goo.gl/PrPgpB
• Slideshare link : http://goo.gl/0HY6ep
• Twitter Page : https://goo.gl/tohkcI
• Instagram page : https://goo.gl/OOGVig
Split ridge and expansion techniques are effective for the correction of moderately resorbed edentulous ridges in selected cases.
Transverse expansion is based on osseous plasticity obtained by corticotomy. It progressively allows for an adequate transversal intercortical diameter large enough to insert one or several dental implants.
The gap created by sagittal osteotomy expansion undergoes spontaneous ossification, following a mechanism similar to that occurring in fractures.
socket shield technique is a modified method of implant placement where many short comings of implant placement can be solved...
it is nothing but retaining of buccal cortical plate during extraction and implant is placed immediatly
The maxillary sinuses were first illustrated and described by Leonardo Da Vinci in 1489 and later documented by the English anatomist Nathaniel Highmore in 1651.
The maxillary sinus, or antrum of Highmore, lies within the body of the maxillary bone and is the largest and first to develop of the paranasal sinuses.
Shape- a pyramid-shaped cavity; base- adjacent to the nasal wall; apex- pointing to zygoma.
Size- insignificant until eruption of permanent dentition; average dimensions of adult sinus- 2.5–3.5 cm wide, 3.6–4.5 cm tall, and 3.8–4.5 cm deep; estimated volume of approximately 12–15 cm.
Extent- Anteriorly, extends to canine and premolar area. sinus floor usually has its most inferior point near the first molar region.
Zygomatic Implants
An inadequate bone support requires Zygomatic Implants.
Although Zygomatic Implants are placed when amount of bone is lesser but it also have some complication.
Few complications, during surgery are Zygomatic bone fracture, orbital penetration, Implant head damage.
Post-operative complications are:- severe fracture, failure of Implant, oro-antral fistula, soft tissue inflammation, sinusitis.
Implant placement needs precise hands, and should be perform by impeccable Implantologist.
Dr. Rajat at Dr. Sachdeva's Dental Institute is deft Implantologist.
Thorough experience of dealing with patients and mentoring student establishing next level Implants Dentistry.
Call us to know more:-
+919818894041,01142464041
Follow our link:-
Google link:
https://business.google.com/dashboard/l/04970356233769420071
Facebook link for Dental Courses:
https://www.facebook.com/dentalcoursesdelhi/
Facebook link for Dental Treatments:
https://www.facebook.com/sachdevadental/
You tube Link:
https://www.youtube.com/user/drrajatsachdeva
Linkedin link:
https://www.linkedin.com/in/drrajatsachdeva/
Slideshare:
https://www.slideshare.net/drrajatsachdeva
Twitter Page :
https://twitter.com/drrajatsachdeva
Instagram page :
https://www.instagram.com/surgicalmasterrajat/
Practo Profile :
https://www.practo.com/delhi/doctor/dr-rajat-sachdeva-dentist
Blogger Profile :
http://drrajatsachdeva.blogspot.com/
Facial Aesthetics Facebook Page :
https://www.facebook.com/facialaesthetics.delhi
Facial Aesthetics you tube channel :
http://www.youtube.com/channel/UCheM4wF9nWGXJYOmScvsQNw
“Program on Ridge Split and Ridge Augmentation for Implant Placement”- Two lectures on “Concepts of Ridge Augmentation” and “Novel and Simpler Approaches to Ridge Augmentation”. Event organized by the Dental Experts and held at Paneenya Mahavidyalaya Institute of Dental Sciences, Hyderabad, India on 18/11/2016.
Indirect Sinus Lift
A sinus lift procedure is essentially done to increase bone height and density in the posterior maxilla.
Extremely effective in increasing bone height. for more details visit our website https://www.implantdentistindia.com/i...
Direct Sinus Lift
The direct sinus lift or the lateral window sinus elevation is a widely used technique when resorption of the alveolar bone which leads to insufficient bone height (No bone to place implant). for more details please visit https://www.implantdentistindia.com/d...
We will assure you of the best treatment in this area.
Experienced Implantologist -Dr. Sudhakar Reddy, a Maxillofacial surgeon by specialization has vast experience with such a surgical procedures and can make this surgery very simple.
Book an appointment now
The Controlled Assisted Ridge Expansion Technique for Implant placement in An...Indian dental academy
Indian Dental Academy: will be one of the most relevant and exciting training
center with best faculty and flexible training programs for dental
professionals who wish to advance in their dental practice,Offers certified
courses in Dental implants,Orthodontics,Endodontics,Cosmetic Dentistry,
Prosthetic Dentistry, Periodontics and General Dentistry.
The biological fixation determines the longevity of dental implant treatment. It ensures the long term survival of dental implant. Better the osseointegration,higher will be the survival rate
Sinus lift with dental implants Placement.(with Clinical Photographs) Dr. ...All Good Things
Hi. This is Dr. Amit T. Suryawanshi. Oral & Maxillofacial surgeon from Pune, India. I am here on slideshare.com to share some of my own presentations presented at various levels in the field of OMFS. Hope this would somehow be helpful to you making your presentations. All the best & your replies are welcomed!
Zygomatic Implants
An inadequate bone support requires Zygomatic Implants.
Although Zygomatic Implants are placed when amount of bone is lesser but it also have some complication.
Few complications, during surgery are Zygomatic bone fracture, orbital penetration, Implant head damage.
Post-operative complications are:- severe fracture, failure of Implant, oro-antral fistula, soft tissue inflammation, sinusitis.
Implant placement needs precise hands, and should be perform by impeccable Implantologist.
Dr. Rajat at Dr. Sachdeva's Dental Institute is deft Implantologist.
Thorough experience of dealing with patients and mentoring student establishing next level Implants Dentistry.
Call us to know more:-
+919818894041,01142464041
Follow our link:-
Google link:
https://business.google.com/dashboard/l/04970356233769420071
Facebook link for Dental Courses:
https://www.facebook.com/dentalcoursesdelhi/
Facebook link for Dental Treatments:
https://www.facebook.com/sachdevadental/
You tube Link:
https://www.youtube.com/user/drrajatsachdeva
Linkedin link:
https://www.linkedin.com/in/drrajatsachdeva/
Slideshare:
https://www.slideshare.net/drrajatsachdeva
Twitter Page :
https://twitter.com/drrajatsachdeva
Instagram page :
https://www.instagram.com/surgicalmasterrajat/
Practo Profile :
https://www.practo.com/delhi/doctor/dr-rajat-sachdeva-dentist
Blogger Profile :
http://drrajatsachdeva.blogspot.com/
Facial Aesthetics Facebook Page :
https://www.facebook.com/facialaesthetics.delhi
Facial Aesthetics you tube channel :
http://www.youtube.com/channel/UCheM4wF9nWGXJYOmScvsQNw
“Program on Ridge Split and Ridge Augmentation for Implant Placement”- Two lectures on “Concepts of Ridge Augmentation” and “Novel and Simpler Approaches to Ridge Augmentation”. Event organized by the Dental Experts and held at Paneenya Mahavidyalaya Institute of Dental Sciences, Hyderabad, India on 18/11/2016.
Indirect Sinus Lift
A sinus lift procedure is essentially done to increase bone height and density in the posterior maxilla.
Extremely effective in increasing bone height. for more details visit our website https://www.implantdentistindia.com/i...
Direct Sinus Lift
The direct sinus lift or the lateral window sinus elevation is a widely used technique when resorption of the alveolar bone which leads to insufficient bone height (No bone to place implant). for more details please visit https://www.implantdentistindia.com/d...
We will assure you of the best treatment in this area.
Experienced Implantologist -Dr. Sudhakar Reddy, a Maxillofacial surgeon by specialization has vast experience with such a surgical procedures and can make this surgery very simple.
Book an appointment now
The Controlled Assisted Ridge Expansion Technique for Implant placement in An...Indian dental academy
Indian Dental Academy: will be one of the most relevant and exciting training
center with best faculty and flexible training programs for dental
professionals who wish to advance in their dental practice,Offers certified
courses in Dental implants,Orthodontics,Endodontics,Cosmetic Dentistry,
Prosthetic Dentistry, Periodontics and General Dentistry.
The biological fixation determines the longevity of dental implant treatment. It ensures the long term survival of dental implant. Better the osseointegration,higher will be the survival rate
Sinus lift with dental implants Placement.(with Clinical Photographs) Dr. ...All Good Things
Hi. This is Dr. Amit T. Suryawanshi. Oral & Maxillofacial surgeon from Pune, India. I am here on slideshare.com to share some of my own presentations presented at various levels in the field of OMFS. Hope this would somehow be helpful to you making your presentations. All the best & your replies are welcomed!
Sinus lift procedure: the maxillary sinus elevation and the bone augmentation procedure is technique sensitive, requiring meticulous surgical skills and expertise.
Connect with me @ https://in.linkedin.com/in/drmaggitom
Implant surgeries to overcome anatomic difficulties ii / dental implant cour...Indian dental academy
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and
offering a wide range of dental certified courses in different formats.for more details please visit
www.indiandentalacademy.com
Sinus Lift and Immediate Implant PlacementDental Evo
Sinus Lift and Immediate Implant Placement, using LAS kit and TS3 implants.
Presentation by Dr Nicola Baldini DDS
http://www.dentalevo.it/dentistry-materials/sinus-lift-big-buccal-window/
http://www.dentalevo.it/dentistry-materials/sinus-lift-small-buccal-window/
1 introduction to guide right compnents single implantDePlaque
Guide Right Surgical Guide System is a system of components for the fabrication and correction of diagnostic and surgical guides in one or two dimensions.
surgical anatomy of nose is a humble attempt to make the anatomy of nose simpler and easy for medical students and fellow physicians. at the end of the presentation the students will be able to identify all the structures.
An Introduction, History, Diagnosis, Current Guidelines on Treatment of trochanteric fractures of femur. Presentation also contain an introduction of Dynamic Hip Screw and Surgical Techniques.
It restore alveolar bone to the level existing at the time of surgery or slightly more apical to this level. Aim is to achieve positive bony architecture.
STEPS INCLUDE:
1.VERTICAL GROOVING
2. RADICULAR BLENDING
3. FLATTENING INTERPROXIMAL BONE
4. GRADUALIZING MARGINAL BONE
PREFERRED TREATMENT FOR ONE WALLED PERIODONTAL BONE DEFECTS (HEMISEPTUM)
�
Pre prosthetic surgery /certified fixed orthodontic courses by Indian dental ...Indian dental academy
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and offering a wide range of dental certified courses in different formats.
Indian dental academy provides dental crown & Bridge,rotary endodontics,fixed orthodontics,
Dental implants courses.for details pls visit www.indiandentalacademy.com ,or call
0091-9248678078
The denture-wearing history should provide information on the age of existing dentures, the frequency of denture replacement, the patient's experiences and expectations. It is important to identify whether any previous dentures have been successful as it may be suitable to copy features from a previously successful set. It will be important to manage expectations for those patients with a history of denture intolerance, yet technically satisfactory prostheses.
Clinical examination
Clinical examination should fully evaluate both the patient's anatomy and previous dentures to anticipate challenges and the potential to improve upon retention, stability, support, appearance and/or other factors. This should be undertaken in a systematic manner and would typically involve assessment of anatomy followed by an assessment of any existing dentures. This should follow a diagnostic process to determine if the patient presents with:
Technically adequate dentures on a favourable tissue base
Technically adequate dentures on an unfavourable tissue base
Technically inadequate dentures on a favourable tissue base
Technically inadequate dentures on an unfavourable tissue base.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
263778731218 Abortion Clinic /Pills In Harare ,sisternakatoto
263778731218 Abortion Clinic /Pills In Harare ,ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group of receptionists, nurses, and physicians have worked together as a teamof receptionists, nurses, and physicians have worked together as a team wwww.lisywomensclinic.co.za/
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
2. Contents
•Introduction
•Anatomy of the maxillary sinus
•Classification of Bone
• Amount of Available Bone
• Misch Classification on Bone Density
• CT Classification
•Classifications of the Posterior Maxilla
• Misch Classification
• Chiaspasco Classification
•Indications and Contraindications
•Sources of Graft material
•Techniques
D.V.BHUVANESH KUMAR 2
3. •Prosthetic Management of the Sinus
Graft Patient
•1st Stage Provisional Prosthesis
•2nd Stage Provisional Prosthesis
•Definitive Prosthesis
•Complications
•Review of Literature
D.V.BHUVANESH KUMAR 3
4. Introduction
A common problem
encountered while
placing implant fixtures
in the posterior maxilla
region is the lack of bone
required for successful
implant therapy
This problem led to the
development of the sinus
elevation procedure by
Tatum, James and Boyd
in the 1950s.
D.V.BHUVANESH KUMAR 4
5. •Grafting of the sinus floor increases the vertical height
of the posterior maxillary bone prior to implant
placement
•The reports of implant survival under functional
loading vary from 36% to 61.7% and the overall
success rate is 91.6% for implants with a rough surface
and 92.3% for particulate bone grafts.
The 1996 Sinus
Consensus
Conference deemed
this therapeutic
modality highly
predictable and
effective
D.V.BHUVANESH KUMAR 5
7. •Is approximately 15ml in
volume air space although
the actual size depends on
the amount of resorption
that has taken place
•Formation begins in the
second to third year of life
and is nearly complete by
8 years of age
•It has a non-physiologic
drainage port high on the
medial wall that drains
into the middle meatus of
the nose.D.V.BHUVANESH KUMAR 7
8. •The bony walls are thin, except for the anterior
wall and the alveolar ridge in the dentate patient.
•Is lined with a pseudostratified columnar
epithelium – “Schneiderian Membrane”
•Beneath the surface epithelium , is a highly
vascular thin tissue which Is followed by
periosteum D.V.BHUVANESH KUMAR 8
9. •Area of sinus surgery is mainly supplied by branches
from the internal maxillary artery.
•Other arteries supplying the sinus are:
• Infraorbital artery
• Superior labial artery
• Anterior ethmoidal arteryD.V.BHUVANESH KUMAR 9
10. Classification of Bone
Division A Bone (Abundant Bone)
Division B Bone (Barely Sufficient Bone)
Division C Bone (Compromised Bone)
Division D Bone (Deficient Bone)
Bone Density
D1 Dense Cortical Bone
D2 Thick dense to porous cortical bone
on crest and coarse trabecular bone
within
D3 Thin porous cortical bone on crest and
fine trabecular bone within
D4 Fine trabecular bone
D5 Immature, non-mineralized bone
D1: >1250 Hounsfield units
D2: 850-1250 Hounsfield units
D3: 350-850 Hounsfield units
D4: 150-250 Hounsfield units
D5: <150 Hounsfield units
D.V.BHUVANESH KUMAR 10
16. Chiapasco Classification (2003)
•Modification of the existing classifications with the aim
of correlating morphology with current surgical
reconstructive protocols.
•Classification is based on 3 variables:
• Width
• Height of the residual alveolus
• Inter-ridge relation
•The variables are used to define 9 types of sinus-
posterior maxillary alveolar morphologies according to
their treatment needs
•Classes A to D address height and width, and the
remaining classes define crown height space.
D.V.BHUVANESH KUMAR 23
17. Class A
•Residual alveolar ridge height of 4 to 8mm
•Residual alveolar ridge width of at least 5mm
(i.e. absence of significant horizontal
resorption and maintenance of acceptable
horizontal intermaxillary relationships)
•Absence of vertical resorption of the
alveolar ridge with maintenance of
acceptable vertical intermaxillary relationship
•Suggested Surgical Protocol:
A. Sinus Elevation with osteotome
technique
B. Sinus Elevation via lateral approachD.V.BHUVANESH KUMAR 24
18. Class B
•Residual alveolar ridge height of 4 to 8mm
•Residual alveolar ridge width of 5mm(i.e. presence
of horizontal resorption and unfavorable
horizontal intermaxillary relationship)
•Absence of vertical resorption of the alveolar
ridge with maintenance of acceptable vertical
interarch distance
•Suggested Surgical Protocol:
A. Sinus Elevation and lateral bone grafting
B. Sinus Elevation and guided bone
regeneration
D.V.BHUVANESH KUMAR 25
19. Class C
•Residual alveolar ridge height of less than 4mm
•Residual alveolar ridge width of at least 5mm (i.e.
absence of significant horizontal resorption with
maintenance of acceptable horizontal
intermaxillary relationship)
•Absence of vertical resorption of the alveolar
ridge with maintenance of acceptable vertical
interarch distance
•Suggested Surgical Protocol:
•Sinus Elevation via lateral approach
D.V.BHUVANESH KUMAR 26
20. Class D
•Residual alveolar ridge height of less than 4mm
•Residual alveolar ridge width of less than
5mm(i.e. presence of horizontal resorption and
unfavorable horizontal intermaxillary relationship)
•Absence of vertical resorption of the alveolar
ridge with maintenance of acceptable vertical
interarch distance
•Suggested Surgical Protocol:
A. Sinus elevation via lateral approach with
lateral bone grafting
B. Sinus Elevation and guided bone
regeneration D.V.BHUVANESH KUMAR 27
21. Class E
•Same characteristics as Class A except with increased
crown height space
•Suggested Surgical Protocol:
A. Vertical onlay grafts with autogenous bone block
B. Interpositional alveolar bone graft
C. Vertical guided bone regeneration
D. Vertical distraction osteogenesis
•The sinus graft is associated with one of these procedures
but only if correction of the vertical intermaxillary
discrepancy is insufficient to obtain adequate bone
volume for implant placement
D.V.BHUVANESH KUMAR 28
22. Class F
•Same characteristics as Class B except with
increased vertical crown height space
•Suggested Surgical Protocol:
A. Simultaneous vertical and horizontal onlay grafts
with autogenous bone blocks
B. Interpositional bone graft without sinus grafting
C. Simultaneous vertical and horizontal bone
regeneration
•Vertical distraction osteogenesis is not indicated
because the technique does not correct the
horizontal defect
D.V.BHUVANESH KUMAR 29
24. Class G
•Same characteristics of Class C except
with increased vertical crown height
space
•Suggested Surgical Protocol:
A. Sinus graft via a lateral approach
combined with vertical autogenous
block onlay graft
B. Sinus graft with vertical guided bone
regeneration D.V.BHUVANESH KUMAR 31
25. Class H
•Same characteristics as class D except with
increased vertical crown height space
•Suggested Surgical Protocol:
A. Sinus graft via a lateral approach with
simultaneous vertical and horizontal onlay
block grafts
B. Sinus graft with simultaneous vertical and
horizontal guided bone regeneration
D.V.BHUVANESH KUMAR 32
29. Pneumatization of the Sinus
•The maxillary sinus retains
its overall size when teeth
remain in function, but it
expands when posterior
teeth are lost.
•The antrum expands both
inferiorly and laterally
potentially invading the
canine and lateral piriform
regions.
•After the loss of teeth, the
amount of teeth in the
posterior maxilla is greatly
reduced. D.V.BHUVANESH KUMAR 39
30. •A major criterion for successful implant treatment is the
amount of available bone. Height of the bone is a
consideration for predictability of implant treatment
•Because of periodontal disease, tooth loss, and sinus
expansion, there is often less than 10mm of bone
between the maxillary sinus floor and the alveolar crest
ridge.
•Removal of teeth in patients
with “pneumatic trifurcation”
can leave only 4 to 5mm
of bone remaining
D.V.BHUVANESH KUMAR 40
31. Poor Bone Density
•Bone mineral density is critically important for
implant survival under a load. Implants are at the
greatest risk of failure under conditions of poor
mineralization.
•The bone density of the maxilla is often 5 to 10
times lower than that of the anterior mandible
and the quality of bone in the posterior maxilla
is poorer than in any other intraoral region
•Deficient osseous structure jeopardizes not only
the initial implant stability but also load bearing
capacity.
D.V.BHUVANESH KUMAR 41
32. Strong Occlusal Forces
•The bite force in the molar region for a dentate
individual ranges from 1,378 to 1,723 Pa.
•Natural molars have a 200% more surface area
than premolars and a significantly wider
diameter. Both these factors reduce bone strain.
•Following this natural model, implant support
should be greater in the posterior molar region
than in any other area of the mouth.
D.V.BHUVANESH KUMAR 42
33. •In addition, the posterior maxilla opposes
natural teeth or implant supported
restorations contributing greater force to
soft tissue-borne restorations.
•Therefore decreased bone quality and
quantity as well as increased bite force
should be considered in the treatment of this
region of the mouth.
D.V.BHUVANESH KUMAR 43
34. Contraindicatio
ns
•A grafting procedure generally does not
interfere with sinus function when performed
on a healthy sinus. However when performed
on an unhealthy sinus, the same procedure will
contribute to fluid stagnation and bacterial
overgrowth, leading to exacerbated sinusitis
•The presence of space occupying masses such
as polyps, tumors and hyperplastic mucosa
represent obstacles to the elevation of the sinus
mucosa.
D.V.BHUVANESH KUMAR 44
36. Potentially Irreversible, Relative Contraindications
•Some anatomic and/or structural alterations of the
nasomaxillary complex may interfere with the normal
ventilation and mucociliary clearance of the maxillary
sinus
•Compensation may occur over time, leaving such
conditions clinically silent or with only mild to moderate,
sometimes intermittent symptoms
•Sinus grafting in these settings decompensate a
compromised sinus, causing mucus stasis, suprainfection
and subacute sinusitis.
•Elevation of the sinus floor and/or modification of the
sinus anatomy may on occasion lead to better sinus
drainage in the presence of mild sinus membrane
dysfunction D.V.BHUVANESH KUMAR 46
37. Irreversible, Absolute Contraindications
1. Severe (noncorrectable) deformities of the maxillary sinus
2. Scarred and hypofunctional sinus mucosa following
trauma of previous operation
3. Radiotherapy of the head and neck area (dose above
45Gy)
4. Chronic recurrent sinusitis with or without polyposis, that
disrupts mucociliary clearance and is unresponsive to
medical or surgical treatment
5. Local expression of a systemic granulomatous disease
such as Wegener Granulomatosis or midline idiopathic
granuloma
6. Sarcoidosis
7. Benign but locally aggressive tumor (amelobastoma,
myxoma)
8. Malignant tumor, both primary and metastatic, deriving
from epithelial, connective, or odontogenic tissue
(squamous cell carcinoma, adenoid cystic carcinoma)D.V.BHUVANESH KUMAR 50
38. Intraoral Contraindications
1. Grossly inadequate oral hygiene or inability to
perform or maintain appropriate oral hygiene
2. Untreated periodontal disease of adjacent
dentition
3. Gross malocclusion and insufficient freeway
space for restoration
4. Severe pathologic parafunctional habit
(clenching or bruxism)
5. Fulminant mucosal disease (desquamative
mucosal disease, erosive lichen planus)
6. Severe Xerostomia
D.V.BHUVANESH KUMAR 51
40. Terms
• Autograft / autologous graft: a graft of tissue derived from
another site in or on the body of the organism receiving it.
• Allograft: graft taken from one human and transplanted into
another
• Alloplastic graft: a graft consisting of an inert material
• Xenograft: a graft taken from a donor of another species
-Glossary of Prosthodontic Terms 8
D.V.BHUVANESH KUMAR 61
41. Autografts
•The advantage of using autologous bone
in sinus grafts offers the following
advantages:
1. Increased bone formation
2. Shorter healing time requirements than
for bone substitutes
3. Possibilities for simultaneous lateral
augmentation
4. Low operator costs
5. No risk of disease transmission
D.V.BHUVANESH KUMAR 62
42. Disadvantages
•Need for a second operative site
•Difficulty in obtaining a sufficient amount of
graft material in some cases (especially in
intra-oral sites)
D.V.BHUVANESH KUMAR 63
45. Graft form & Maximum volume
available from autogenous bone
donor sites
Donor Site Form Available Maximum Volume (ml)
Extraoral
Posterior Iliac Crest Block / particulate 140
Anterior Iliac Crest Block / Particulate 70
Tibia Particulate 20 to 40
Cranium Dense cortical Bone 40
Intraoral
Ascending Ramus Block 5 to 10
Anterior Mandible Block / particulate 5
Tuberosity Particulate 2-4
Misc (suction traps) Particulate Varies
D.V.BHUVANESH KUMAR 66
46. Maxillary Tuberosity and Buttress
•Approximate Resorption time: 3-6
months
•Can be used for small reconstructions
with low or moderate osteogenic
potential
•hyperpneumatized unilateral maxillary
sinuses or
•bilateral sinuses in conjunction with other
graft materials
D.V.BHUVANESH KUMAR 67
48. Mandibular Symphysis
•Approximate Resorption time: 4-8
months
•Can be used for small reconstructions
with low or moderate osteogenic
potential
•hyperpneumatized unilateral maxillary
sinuses or
•bilateral sinuses in conjunction with other
graft materials
D.V.BHUVANESH KUMAR 69
51. Mandibular Ramus and Bone Shavings from
Adjacent Areas of Surgical Site
•Approximate Resorption time: 3-7 months
•Can be used for small reconstructions with
low or moderate osteogenic potential
•hyperpneumatized unilateral maxillary sinuses
or
•bilateral sinuses in conjunction with other graft
materials
D.V.BHUVANESH KUMAR 74
54. Bone Suctioned while Drilling Osteotomies
•Approximate Resorption Time: 1-3
months
•Very small defects such as exposed
implant threads
D.V.BHUVANESH KUMAR 79
56. Advantages
•Ready availability
•Elimination of the need for a patient
donor site
•Reduced anesthesia and surgical time
•Decreased blood loss
•Fewer complications
D.V.BHUVANESH KUMAR 86
57. Hydroxyapat
ite
•Hydroxyapatite in its various permutations has
demonstrated excellent osteoconductive capacity.
•Marorana et al compared the degree of marginal
bone resorption and implant longevity when HA or
xenograft was used in sinus augmentation and found
no significant difference in terms of bone resorption
around implants or osseointegration success rates in a
4-year follow-up study.
•They reported a 97% success rate for treatment of 34
patients with 26 sinus grafts and 37 implants placed,
with 1 implant lost.
D.V.BHUVANESH KUMAR 87
58. •Silva et al used HA in the form of solid
bioceramic discs to treat critical-sized
defects in rat craniums that were
allowed to heal primarily. They found
that the ceramic achieved better results
than autogenous grafts alone.
D.V.BHUVANESH KUMAR 88
59. Bioactive Glass
•Bioglass is a silicon dioxide material that
contains calcium, phosphate and sodium ions
(45% SiO2, 24.5% CaO, 24.5% Na2O and 6%
P2O5) in particle sizes ranging from 90 to 710µm
•When bioglass particles come into contact with
tissue fluid, hydroxycarbonate (HCA) forms on
their surface, making them highly conducive to
osteoblast attachment via chondroitin sulfate
and glycosamine protein bonds.
•Mineralization progresses rapidly under these
conditions, resulting in dense bone formation.
D.V.BHUVANESH KUMAR 89
60. •Bioactive glass bonds directly to bone.
•Through osteoconduction, glass becomes
wholly incorporated and is then resorbed
and replaced by bone.
D.V.BHUVANESH KUMAR 90
61. Beta-tricalcium Phosphate
•β-TCP is a highly biocompatible, resorbable,
osteoconductive grafting material that has been tested
in many animal studies and used extensively for repair
of bone defects and to expand autograft for sinus
grafting.
•Artzi et al placed β-TCP and bovine bone in critical sized
defects in dog mandibles. Both showed excellent bone
bridging, but the β-TCP had entirely resorbed by 24
months and was completely replaced by lamellar bone.
•Engelke et al used β-TCP to place sinus-directed
implants and reported that 200 implants
osseointegrated for a 95% success rate.
D.V.BHUVANESH KUMAR 91
63. D.V.BHUVANESH KUMAR 93
• 100% synthetic and fully Resorbable.
• It is composed of calcium phosphosilicate (CPS) particles in a bimodal size
distribution combined with
• polyethylene glycol and glycerine binder.
64. •Upon implantation, the water soluble binder is
•absorbed within 24 to 72 hours, creating a 3-
dimensional porous scaffold that facilitates
diffusion of blood and tissue fluids through the
matrix
•After implantation, surface reactions result in
absorption of the graft material, a controlled
release of Si, Ca, and P ions, and concurrent new
bone formation.
•These surface reactions result in an
osteostimulative effect, defined as the stimulation
of osteoblast proliferation in vitro as evidenced by
increased DNA content and elevated osteocalcin
and alkaline phosphatase levels
D.V.BHUVANESH KUMAR 94
66. Sinus Allograft
Procedures
•Allogenic bone is placed using any of
the three generally accepted
procedures:
•The osteotome technique
•The simultaneous sinus elevation and
implant placement technique
•A two stage lateral approach to sinus
elevation and implant placement
D.V.BHUVANESH KUMAR 110
67. Osteotome Technique
•Was developed to
compress soft maxillary
bone
•Improved initial fixation
obtained from bone
compression of the
osteotomy walls leads
to better primary
stabilization.
•Healing is rapid and
uneventful
D.V.BHUVANESH KUMAR 111
68. •Requires a two-person team
•Involves inserting a series of osteotomes of successful
larger diameter until full depth is reached, if possible.
D.V.BHUVANESH KUMAR 112
69. •Surgeon positions and guides the instrument
with both hands – one hand creates a rest
and maintains stability while the other hand
gently rotates and applies pressure with the
osteotome
•The assistant will apply gentle malleting
technique to the osteotome.
•Osteotome is roated after every stroke to
prevent binding to the bone.
•Osteotomes are to be kept lubricated but
irrigation is not required.
D.V.BHUVANESH KUMAR 113
70. •To form a round osteotomy, side to side
movement of the instrument is to be avoided.
•Each strike of the mallet is applied to the
osteotome in exactly the same path that it is held.
Off-angled malleting causes the osteotome to
migrate and creates an elliptical osteotomy,
which comprimises initial fixation
•The surgeon places restraining pressure on the
osteotome to prevent it from advancing more
than 1mm with each impact of the mallet
•A drill can be used at any step to increase the
diameter of the osteotomy or deepen the
preparation as needed.
D.V.BHUVANESH KUMAR 114
74. Staged Sinus Floor
Elevation
•A technique for sinus floor augmentation with
delayed implant placement
•Introduced by Tatum in 1977
•Large sized osteotome is used to infracture the
crest after limited use of drills or trephines
•Grafting is done without disturbing the sinus
membrane. A collagen membrane is used to
close the sinus membrane
•The crestal entry creates a “socket” that heals
rapidly.
•Implant fixture is placed 6 months later
D.V.BHUVANESH KUMAR 118
75. Lateral Wall Approach for Sinus
Elevation
•Is used for both delayed and simultaneous
implant placement
•Autogenous bone is harvested from the
lateral wall of the antrum for use in
conjunction with the allograft
•The full extent of the sinus wall is made
visible by thinning out of the lateral wall
•Osteotomy is performed using a multifluted
finishing bur.
•Infracture and membrane elevation are
accomplished and the graft procedure is
performed. D.V.BHUVANESH KUMAR 119
76. a. Delayed sinus elevation with 1 to 4mm of residual bone. A partial thickness
Flap is bevelled to the palate
a. Elevation of Buccal and Palatal flaps & osteotomy made in the lateral wall
of sinus D.V.BHUVANESH KUMAR 120
80. Diagnosis and Treatment Planning
•Verify the maxillomandibular relationship
using mounted casts
•Duplicate the casts and fabricate a wax
mockup to determine the prospective
occlusal plane, occlusal scheme and
esthetics
•Make impression of the mockup to create
surgical template and a provisional
prosthesis and to aid in the creation of both
the second stage screw-retained provisional
restoration and the definitive prosthesis.
D.V.BHUVANESH KUMAR 124
81. First Stage Provisional Prosthesis
•Removable Partial Denture
•Used to replace teeth distal to the canine
•Must have maximum stability and cross
arch transmission of occlusal forces
• Retaining system should include shallow occlusal or
incisal rests as well as retaining and bracing arms
• A combination clasp system provides stress relief and
also permits easy adaptation and subsequent
adjustment of the retainer system to the abutment
teeth
• Provide relief over the edentulous areas
D.V.BHUVANESH KUMAR 125
82. •Pressure from the transitional CPD may cause
micromovement of the implants – the patient
should be instructed not to wear the
prosthesis for 3 weeks following implant
surgery. At the time of insertion, the denture
flange must be kept away from the graft area
•The prosthesis will be worn for at least 9
months. Following 1st stage surgery, it will be
refitted and the tissue treatment material will
be replaced weekly until the surgical site has
healed.
D.V.BHUVANESH KUMAR 126
83. Second Stage Provisional
Prosthesis
•Following implant uncovering and abutment
installation, a screw-retained fixed-detachable
prosthesis is fabricated.
•The prosthesis is fabricated as soon as it is
feasible following installation of the preselected
abutments
•It permits loading of the grafting material and
surrounding alveolar bone without going directly
to the final restoration
•Provisional loading allows the graft and native
alveolar bone to remodel in response to bone
strains transmitted to through loadingD.V.BHUVANESH KUMAR 127
84. •The provisional prosthesis is worn for at
least 6 months
•When anterior implant(s) are in ungrafted
alveolar bone and posterior implants are in
the sinus graft, the definitive prosthesis is
constructed approximately 6 months after
placement of the second-stage provisional
prosthesis.
•If the prosthesis is supported only by
implants placed in a graft material, the
provisional is worn for 1 year prior to the
fabrication of the definitive prosthesis to
allow for maturation of the graft.
D.V.BHUVANESH KUMAR 128
85. Advantages
•The advantages of using a second-stage single
screw-retained provisional prosthesis are:
•Acts a template for the definitive prosthesis
•Allows the patient to wear a fixed prosthesis after
second-stage surgery
•Allows the patient to learn how to function with
and maintain a screw-retained fixed detachable
prosthesis
•Is retained by the patient after completion of the
definitive prosthesis, and may be used if
alterations to the final prosthesis are ever
required
D.V.BHUVANESH KUMAR 129
86. Definitive Prosthesis
•Is a fixed-detachable screw retained restoration
constructed from type IV gold alloy with a heat-
cured acylic resin veneer
•For shock absorption, acrylic resin occlusal surfaces
may be employed to reduce forces on the
underlying graft and implants.
•When < 5mm of residual bone remained beneath
the sinus before grafting use acrylic resin occlusal
surfaces
•When > 5mm residual bone was present beneath
the sinus, gold occlusal surfaces are used.
D.V.BHUVANESH KUMAR 130
92. Tarnow DP, Wallace SS, Froum SJ. Histologic and clinical
comparision of bilateral sinus floor elevations with or without
barrier membrane Int J. Periodontics Restorative Dent 2000
A controlled trial by Tarnow et al, Tawil and Mawla and Froum
et al showed that there is a higher implant survival rate with
membrane use.
Study Survival Rate with Survival Rate
without
Tarnow et al
(2001)
100%; n =28
implants
92.6%; n = 27
implants
Tawil et al (2001) 93.1%; n = 29
implants
78.1%; n=32
implants
Froum at al (1998) 99.2%; n= 133
implants
96.3%; n=82
implants
D.V.BHUVANESH KUMAR 147
93. Tepper G. et al: Effects of sinus lifting on voice quality: a prospective
study and risk assessment. Clin. Oral Impl. Res. 14, 2003; 767–774
•No changes were detected in any of the commonly
evaluated parameters.
•These were rated subjectively by patients and their
friends or relatives and objectively with
instrumental tools under isolated phoniatric lab
conditions.
•They concluded that, sinus lift surgery appears to be
a safe, predictable evidence-based method for
regenerating the highly atrophic posterior maxilla,
which does not jeopardize the individual
characteristic voice pattern of high-profile patients
critically dependent on their voices for their
livelihood
D.V.BHUVANESH KUMAR 151
94. D.V.BHUVANESH KUMAR 152
Dec-2013
There were 197 implants placed and mean age of the group
was 40.2 ± 10.7 years. There was a slight male predilection
(54.3%).
The gain in bone height as expressed in percentage after a
year was 134.6%. On comparing the length of residual alveolar
bone (RAB) at start and end of study, ISAT had a mean
preoperative height of 7.88 mm while postoperative
height was 13.22 mm.
For DSAT, the mean height at start of treatment was 3.94
mm while at the end it was 10.13 mm. Themean increase in
height was 6.19 mm
95. •Age, gender, and period of edentulism did
not influence the outcome.
• The alveolar width appears to differ and
influence the outcome.
•When alveolar width increases, wider
diameter implants can be placed by
compromising height.
•Thus it is a clinical experience that would be
extremely helpful to gauge the outcome of
the condition.
D.V.BHUVANESH KUMAR 153
96. • Jenson OT: The Sinus Lift Procedures. 2° Edition, Mosby Co. 2007
• Misch CE: Contemporary Implant Dentistry. Mosby Co. 1997
• Garg A: Bone: Harvesting Biology and Grafting.
• Babbush CA: Implant dentistry – the art and science.
D.V.BHUVANESH KUMAR 157