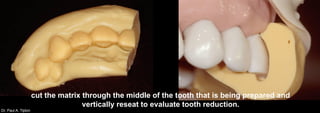
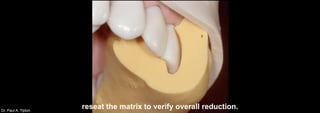
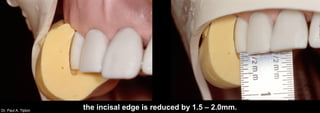
Dr. Paul A. Tipton discusses different techniques for preparing teeth for porcelain veneers. For a conventional veneer on the upper right first tooth, preparation involves 0.5mm labial reduction and removing 2mm from the incisal edge. A putty matrix is used as a guide. For a butt joint veneer on the upper right second tooth, the labial surface is reduced by 0.3-0.5mm and 1.5-2mm removed from the incisal edge, which is prepared at a 30 degree angle. Slice preparations are used to address imbrication, rotation, diastemas or missing papillae, reducing the labial surface by 0.3-0