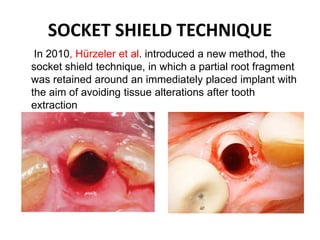
The document discusses the socket shield technique for implant placement, which preserves a portion of the tooth root to minimize tissue alterations post-extraction. It outlines the process, indications, and contraindications for this technique while highlighting its advantages and potential disadvantages. The technique is particularly beneficial for preserving the buccal bone in cases of thin cortical plates, making it a viable alternative to other surgical augmentations.