Paranasalsinuses
•
35 likes•8,330 views

Paranasal sinuses are air-filled spaces located around the nose. This document discusses the anatomy, physiology, development, and pathologies of the paranasal sinuses. It describes the examination and investigations used to evaluate sinus diseases. The major classifications of sinus pathologies discussed are developmental variations, inflammatory/infectious diseases, cysts, tumors, and other surgically relevant conditions. Specific conditions like polyps, sinusitis, and granulomatous diseases are described in more detail.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (14)
Similar to Paranasalsinuses
Similar to Paranasalsinuses (20)
More from Cathrine Diana
Recently uploaded
Recently uploaded (20)
Paranasalsinuses
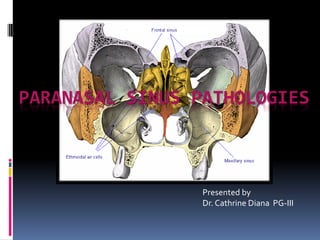
- 1. PARANASAL SINUS PATHOLOGIES Presented by Dr. Cathrine Diana PG-III
- 2. contents Paranasal sinuses Introduction Development Anatomy Physiology Examination and investigations Paranasal sinus pathologies Classification Description Complications Treatment
- 3. INTRODUCTION Sinus (Latin) - fold or pocket. Paranasal sinuses - four paired, hollow air filled spaces in various cranio-facial bones Named after the bones in which they are located
- 4. INTRODUCTION Clinically, Divided into two groups: 1. Anterior group: maxillary, frontal, anterior and middle ethmoidal air cells. They all open in the middle meatus. 2. Posterior group: Posterior ethmoidal and the sphenoid sinus
- 5. DEVELOPMENT Excavation of bone by air-filled sacs (pneumatic diverticula) from the nasal cavity. Begins prenatally - continues through lifetime.
- 7. ANATOMY– MAXILLARYSINUS MAXILLARY ANTRECHEA / ANTRUM OF HIGHMORE Largest Maxilla - under the eyes, on either side of the nose. Pyramidal - base toward the lateral wall of nose and apex directed laterally into the zygomatic process. Capacity of 15 ml (average).
- 8. FRONTAL SINUS Situated deep to the inner and outer table of frontal bone Drain- frontal recess to the middle meatus Absent on one (15 %) or both sides (5 %) Drainage pathway – naso- frontal duct- frontal recess - situated at its floor – drains into middle meatus (62%) or ethmoid infundibulum (38%).
- 9. Ethmoid sinus Thin-walled air cavities in the lateral masses of ethmoid bone, between nose and the eyes. 1. Anterior ethmoidal air cells –3- 11 drain into either the ethmoidal infundibulum or the frontonasal duct. 2. Bullar cells (middle ethmoidal air cells) - usually <3 - open in ethmoidal infundibulum. 3. Posterior group :- Up to 7 - usually drain by a single orifice into the superior meatus.
- 10. Agar nasi cells They are the most anterior ethmoidal air cells. . Its size influence the patency of the frontal recess and the anterior middle meatus. Haller cells: Also called infraorbital ethmoid cells. Present in approx. 20 % pateints. Clinical significance – Become infected , with potential extension into orbit. Narrows the maxillary ostium.
- 11. Onodi cells These are posterior ethmoidal cells extending into the sphenoid bone ,either adjacent to or impinging upon the optic nerve. When these Onodi cells abut or surround the optic nerve, the nerve is at risk when surgical excision of these cells is performed. It is also a potential cause of incomplete sphenoidectomy.
- 12. SPHENOID SINUS Body of sphenoid - behind the nose, in the center of the skull. Rarely symmetrical and separated by a thin bony septum. Ostium of the sphenoid sinus is situated in the upper part of its anterior wall and drains into sphenoethmoidal recess. Average size – 2 x 2 x 2 cm. According to Congdon sphenoid pneumatization can be as follows Conchal – 5 % Presellar – 23 % Post-sellar – 67%
- 13. ANATOMY- LATERAL NASALWALL 3 projections - superior, middle and inferior concha. Meatus - space below each concha. Inferior meatus: nasolacrimal duct Middle meatus: Maxillary sinus Frontal sinus Anterior ethmoid sinuses Superior meatus: posterior ethmoid sinuses Sphenoethmoidal recess: sphenoid sinus
- 14. OSTEOMEATAL COMPLEX It is a common channel that links the frontal sinus, anterior and middle ethmoid sinuses and the maxillary sinus to the middle meatus. It is composed of five structures: Maxillary ostium Infundibilum Ethmoidal bulla Uncinate process Hiatus semilunaris
- 15. PHYSIOLOGY– SINUS EPITHELIUM Respiratory epithelium - ciliated pseudostratified columnar epithelium, goblet cells, and submucosal glands Produce a protective mucous blanket - traps bacteria and noxious materials, which are carried by ciliary motion to the ostium and into the nose for elimination
- 16. Ciliary movements: 50- 300 cilia/ cell; 8-20 beat/ second. For maximum ciliary activity: Humidity: >85%, Temperature: 18- 40 degree C, pH: 7- 8. The orientation of the cilia within a given sinus is specific as secretions are propelled towards the natural sinus ostia and from there to the nasopharynx and oropharynx where they are subsequently cleared by swallowing.
- 17. SINUS HEALTH Composition of gas content in the maxillary sinus is similar to venous blood, with high CO2 and lower O2 level compared to breathing air. Sinus health depends on: 1. Mucous secretion of normal viscosity, volume, and composition 2. Normal muco-ciliary flow to prevent mucous stasis and subsequent infection 3. Open sinus ostia to allow adequate drainage and aeration. Negative factors: Dryness of air, Cigarette, Temperature variations, hypoxia, hypercapnia, Hypertonic/ hypotonic fluids, Dehydration, pH changes, diseases (like Cystic fibrosis and Primary ciliary dyskinesia), Drugs (phenylephrine, adrenaline, lidocaine, atropine, antihistaminic), Infections, Anatomic obstruction (septal deviation, enlarged or irregular turbinate), Foreign bodies and Nasal polyps.
- 18. PATHOPHYSIOLOGICALSTAGES OF SINUS DISEASES Initial phase: - reversible Ostium obstruction phase Bacterial phase Chronic phase
- 19. Osteomeatal complex obstruction ↓ Decreased ventilation of the sinuses ↓ Decreased drainage of the sinuses ↓ pO2 decrease, pCO2 increase, mucous stasis ↓ Inflammation and viscous mucous, ciliary movement slowing ↓ Stasis and proteolytic enzymes ↓ Ciliary damage ↓ Anaerobic microorganisms ↓ More damage
- 20. FUNCTIONS OF SINUS 1. Reduction of weight of skull 2. Increasing resonance of the voice 3. Providing a buffer against blows to the face. 4. Insulating sensitive structures like dental roots and eyes from rapid temperature fluctuations in the nasal cavity. 5. Humidifying and heating of inhaled air because of slow air turnover in this region. 6. Regulation of intranasal and serum gas pressures 7. Increasing surface area for olfaction 8. Contribute to facial growth
- 21. EXAMINATION History and systemic clinical examination: Check general signs of health Systemic medical history, history of allergies, drug use and abuse Occupation history Examination of and neck for lumps or swollen lymph nodes
- 22. Examination Local examination of the nose, face, and neck: 1. Anterior Rhinoscopy: Examination of nose with a nasal speculum to check for abnormal areas, useful in evaluation of nasal obstruction. 2. Posterior rhinoscopy: With a mouth mirror in the nasopharynx
- 23. Examination - transillumination Normal transillumination decreases chance of pus in the sinus. No light reflex suggests mucopurulent material or thickening of nasal mucosa. Inexpensive screening tool
- 24. Transillumination of Frontal Sinus Transillumination of Maxillary Sinus 24
- 25. Examination - endoscopy Endoscopic examination/ Rhinoscopy: nasoscope/rhinoscope is a thin, tube-like instrument with a light and a lens for viewing. A special tool on the nasoscope may be used to remove samples of tissue. The tissues samples are viewed under a microscope by a pathologist.
- 26. EXAMINATION – PLAIN RADIOGRAPHS Plain radiographs: to check for Sinus opacifications, Air-fluid level, Mass, Fractures Caldwell view: PA view/ “forehead-nose” view to evaluate maxilla, maxillary and frontal sinus, ethmoid air cells, lamina papyracea
- 27. Water’s view: chin-nose” or “occipito- mental” view for evaluation of the paranasal sinuses. submento-vertical” view to evaluate the sphenoid, the posterior ethmoids, the maxillary and frontal sinuses
- 28. CT SCANS CT scans: Excellent views of the sinuses, best for osteomeatal complex and ethmoidal disease “Limited CT Evaluation” – slice 3-4 mm CT navigation: A computer is used to identify the 3- dimensional location of a probe tip placed within the patient's nose or sinuses.. Improves anatomical identification and avoid damage to vital neighbouring structures such as the brain and eyes.
- 29. AXIAL CT
- 32. CORONAL CT
- 35. SAGITTAL CT
- 36. EXAMINATION MRI: Excellent soft tissue definition - evaluation of neoplastic disease. MRI (magnetic resonance imaging) with gadolinium: Gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture.
- 37. PET scan (positron emission tomography scan): A small amount of radioactive glucose is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. Stuckensen and colleagues found a sensitivity of 70%, 84%, and 66% and a specificity of 82%, 68%, and 74% for PET, ultrasound, and CT scan in terms of nodal metastasis
- 38. 9. Histological examination: Fine-needle aspiration (FNA) biopsy, Incisional biopsy and excisional biopsy are done from pathologic tissues. 10. Culture examination: Correlation of routine nasal culture and sinus culture is poor. Endoscopically guided aspiration of cultures from medial meatus do correlate with sinus culture. Silver stained section showing invasive fungal sinusitis (aspergillus) Allergic mucin of allergic fungal sinusitis
- 39. Classification DEVELOPMENTAL VARIATIONS AND ANOMALIES INFLAMMATORY/INFECTIOUS DISEASES CYSTS TUMORS OTHER SURGICALLY RELEVANT CONDITIONS
- 40. Developmental variations and anomalies Paradoxical curvature of middle turbinate Concha bullosa in middle turbinate Lateralization and pneumatisation of uncinate process Variations of ethmoidal roof anatomy Bulla ethmoidalis – torus ethmoidalis and giant bulla Others: Agenesis of sphenoid sinus, pneumatisation of greater wings of sphenoid and crista galli.
- 41. DEVELOPMENTALVARIATIONSAND ANOMALIES Paradoxical curvature: Normally the convexity of the middle turbinate is directed medially toward the nasal septum. When the convexity is directed laterally, it is termed a paradoxical middle turbinate . Most authors agree that the paradoxical middle turbinate can be a contributing factor to sinusitis.
- 42. DEVELOPMENTALVARIATIONS ANDANOMALIES Concha bullosa: When pneumatization involves the bulbous portion of the middle turbinate it is termed concha bullosa. If only the attachment portion of the middle turbinate is pneumatized, it is termed lamellar concha . A concha bullosa may obstruct the ethmoid infundibulum.
- 43. Variations of uncinate process The uncinate process may be medialized, lateralized, or pneumatized/bent. Medialization occurs with giant bulla ethmoidalis. Lateralization of the uncinate process may obstruct the infundibulum. Pneumatization (uncinate bulla) can rarely cause obstruction of the infundibulum.
- 44. Variation of the ethmoidal roof anatomy The ethmoid roof is of critical importance for two reasons. most vulnerable to iatrogenic cerebrospinal fluid leaks. anterior ethmoid artery is vulnerable to injury. The depth of the olfactory fossa is determined by the height of the lateral lamella of the cribriform plate. In 1962, Keros classified the depth of the olfactory fossa into three types, that is, Keros type I: <3 mm Keros type II: 4-7 mm Keros type III: 8-16 mm - most vulnerable to iatrogenic injury.
- 45. Variations of sphenoid sinus … Agenesis of sphenoid sinus Pneumatisation of other bones The crista galli is normally bony. When aerated, it may communicate with the frontal recess, causing obstruction of the ostium and thus lead to chronic sinusitis and mucocele formation
- 46. Bullae ethmoidalis The bulla ethmoidalis is a prominent anterior ethmoid air cell. Failure to pneumatise - torus ethmoidalis. A 'giant bulla' may fill the entire middle meatus and force its way between the uncinate process and the middle turbinate.
- 47. INFLAMMATORY/ INFECTIOUS CONDITIONS POLYPS SINUSITIS GRANULOMATOUS DISEASES
- 48. POLYPS They are fleshy outgrowths of the nasal mucosa that form at the site of dependent edema in the lamina propria of the mucous membrane, usually around the ostia of the maxillary sinuses. usually start near the ethmoid sinuses and grow into the open areas. Large polyps can block the sinuses or nasal airway. Risk factors: Aspirin sensitivity (wheezing), Asthma, Acute and Chronic sinus infections, Cystic fibrosis, Hay fever (allergic rhinitis).
- 49. Clinical features: Nasal obstruction and mouth breathing Nasal congestion and postnasal drainage Anosmia, hyposmia Sneezing, rhinorrhea Facial pain Ocular itching Bleeding polyps occur in rhinosporidiosis Unilateral polyps occasionally occur in association with or represent benign or malignant tumors of the nose or paranasal sinuses, or in response to a foreign body. Diagnosis: physical examination - A developing polyp is teardrop-shaped; when mature, it resembles a peeled seedless grape. CT scans
- 50. Treatment 1. Steroids –may shrink or eliminate polyps Topical corticosteroid spray - mometasone [30 mcg/spray], beclomethasone [42 mcg/spray], flunisolide - given as 1 or 2 sprays bid in each nasal cavity 1-wk tapered course of oral corticosteroids. 2. Surgery : FESS Steroid therapy after surgery - to retard recurrence. In severe recurrent cases- maxillary sinusotomy or ethmoidectomy, usually done endoscopically. 3. Removal of etiology – control of underlying allergy or infection.
- 51. SINUSITIS Definition: Sinusitis is the inflammatory condition of the mucous membrane lining of the sinuses RHINOSINUSITIS is a better term because: Allergic or non-allergic rhinitis nearly always precedes sinusitis Sinusitis without rhinitis is rare Nasal discharge and congestion are prominent symptoms of sinusitis Nasal mucosa and sinus mucosa are similar and are contiguous
- 52. Classifications ACCORDING TO DURATION: 1. Acute :infection lasting 4 weeks, symptoms resolve completely resolved in < 30 days. 2. Subacute :infection lasting between 4 to 12 weeks, yet resolves completely. 3. Recurrent: ≥ 4 discrete acute episodes per year, each completely resolved in < 30 days but recurring in cycles, with at least 10 days between complete resolution of symptoms and initiation of a new episode 4. Chronic: symptoms lasting more than 12 weeks.
- 53. ACCORDING TO PATHOGEN: 1. Bacterial: Hospital-acquired acute infections are more often bacterial, typically involving Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa 2. Viral: In immunocompetent patients - in the community is almost always viral (eg, rhinovirus, influenza, parainfluenza). antibiotics given for: Mild to moderate sinus symptoms persisting for ≥ 10 days Severe symptoms (eg, fever ≥ 39°, severe pain) for ≥ 3 to 4 days Worsening sinus symptoms after initially improving from a typical viral URI ("double sickening" or biphasic illness)
- 54. 3. Fungal: Usually seen in immunocompromised patients because of poorly controlled diabetes, neutropenia, or HIV infection. It is clinically of 2 types: Non-invasive fungal sinusitis: Saprophytic fungal infestation/colonization Allergic fungal rhinosinusitis (AFRS) Saprophytic fungus balls (mycetoma) Invasive fungal sinusitis – Chronic invasive fungal sinusitis Granulomatous invasive fungal sinusitis Acute (fulminant) invasive fungal sinusitis
- 55. sinusitis According to source: Primary Secondary According to number of sinuses involved: Hemisinusitis –all sinuses on one side Polisinusitis – several sinuses, but not all, are involved Pansinusitis According to source of infection: Rhinogenous Odontogenic Traumatic Hematogenic Allergic
- 56. Risk factors: 1. Obstruction to drainage: most important 2. Defect of self-cleaning mechanism of the mucous membrane of sinus – infections causing immobility of the cilia, Increased viscosity of secretions, Immotile cilia syndrome, Prolonged exposure to cigarette smoke 3. Medications First generation antihistamines (non sedating do not affect) Anticholinergics, Aspirin, Anesthetic agents, Benzodiazepines 4. Immunodeficiency: Immunoglobulin deficiency (IgA, IgG), diabetes, HIV infection 5. Other factors: prolonged ICU stays, severe burns, cystic fibrosis, and ciliary dyskinesia.
- 57. Clinical Features: 1. Nasal congestion and discharge 2. Sore throat and postnasal drip 3. Pain or pressure. 4. Oedema of facial tissues. 5. Bad breath or loss of smell (hyposmia/anosmia). 6. Systemic symptoms: Malaise may be present. Fever and chills suggest an extension of the infection beyond the sinuses, rise in temperature, bad appetite, sleep disturbances, changes of the blood (leukocytosis), Productive cough (especially at night) 7. Complications – ocular, neurological, local
- 58. Diagnosis 1. Diagnosis is clinical; 2. CT and cultures - mainly for chronic, refractory, or atypical cases. 3. X-rays of the apices of the teeth Clinical diagnostic criteria include 2major factors, I major and 2 minor factors or presence of pus in nasal cavity. Major Factors Minor Factors Facial pain/pressure Headache Facial congestion/fullness Maxillary dental pain Nasal drainage/discharge Cough Postnasal drip Halitosis Nasal obstruction/blockage Fatigue Hyposmia/anosmia Ear pain/ pressure/ fullness Fever (acute sinusitis only) Fever Purulence in nasal cavity on examination (diagnostic by itself)
- 59. TREATMENT OPTIONS MEASURES TO ENHANCE DRAINAGE: 1. Heat therapy: Steam inhalation; hot, wet towels over the affected sinuses; and hot beverages 2. Topical vasoconstrictors/ Nasal decongestants: Topical nasal sprays (limit use to 3-7 days) - Phenylephrine, Oxymetazoline, Naphthazoline, Tetrahydrozoline, Zylometazoline. Phenylephrine(0.25%) spray q 3 h or oxymetazoline q 8 to 12 h, are effective but should be used for a maximum of 5 days or for a repeating cycle of 3 days on and 3 days off until the sinusitis is resolved CORTICOSTEROIDS: Corticosteroid nasal sprays can help relieve symptoms but typically take at least 10 days to be effective 3. Systemic vasoconstrictors: Systemic vasoconstrictors, such as pseudoephedrine 30 mg po (for adults) q 4 to 6 h, are less effective.
- 60. 4. Nasal irrigation: Commercial buffered sprays, Bulb syringe, waterpik and ceramic irrigators with lavage tip or disposable enema bucket Washes away irritants and moistens the dry nose. cumbersome and uncomfortable - better for patients with recurrent sinusitis. ANTIHISTAMINICS: recommended if allergy present. They can be oral or topical HYDRATION
- 61. 5. Mucoactive drugs: main purpose - increase the ability to expectorate sputum and/or decrease mucus hypersecretion. 1. Expectorants: hypertonic saline, iodine containing compounds, guaifenesin (glyceryl guaiacolate), ion channel modifiers (tricyclic nucleotides) 2. Mucoregulators: carbocysteine, anticholinergic drugs, glucocorticoids, macrolide antibiotics 3. Mucolytics: classic mucolytic (N-Acetyl Cysteine), peptide mucolytic, non destructive mucolytics 4. Mucokinetics: bronchodialators, ambroxol
- 62. a) Nebulization: best form of physiotherapy. Can be done using compressors or ultrasonic nebulisers. Normal saline solutions are nebulized which has a hydrating effect on the mucous lining. Ultrasonic nebulisers can set the rate according to need. b) Laser therapy: used directly over the sinuses to reduce inflammation c) Ultrasound therapy: sound waves are conducted through a hypoallergenic gel to reduce inflammation and loosen the accumulated mucous. d) Short-wave diathermy e) Rinoflow therapy: new option, basically micronized endotracheal wash. Used in sinusitis, rhinitis, pharyngitis, laryngitis and secretory otitis media.
- 63. Antibiotics and antifungal drugs: Amoxicillin 500 mg tid for 10-14 days - First line Beta-lactanase resistance - Amoxicillin/clavulanate, Cefuroxime, Cefpodoxime, Cefprozil
- 65. Surgery Indications: Sinusitis unresponsive to antibiotic therapy Necrotic sinusitis Orbital complications (abscess and phlegmon of orbit) Intracranial complications (meningitis, brain abscess) Rhinogenic sepsis Odontogenic sinusitis combined with maxillary osteomyelitis. Approaches: 1. Removal of etiology 2. Fess 3. Caldwell-luc procedure 4. Intranasal antrostomy 5. Radical surgeries
- 66. Removal of etiology: Treatment of affected tooth. Caldwell luc approach may be used. Intra-nasal antrostomy may be needed.
- 67. Caldwell - luc Caldwell-Luc is the fenestration of the anterior wall of the maxillary sinus and the surgical drainage of this sinus into the nose via an antrostomy. a middle meatus antrostomy is being utilized as a more physiologic antrostomy..
- 69. FESS: Functional endoscopic sinus surgery (FESS) is the mainstay in the surgical treatment of sinusitis and nasal polyps, including bacterial, fungal, recurrent acute, and chronic sinus problems. Nasal endoscopes through the nostrils to avoid cutting the skin. Telescope diameters - 4mm (adult use) and 2.7mm (pediatric use) Viewing angles - 0 degrees to 30, 45, 70, 90, and 120 degrees Carry: High definition cameras attached to monitors, tiny articulating instruments - cutting, suction, biopsy, curettage All the sinuses can be accessed at least to some degree by means of FESS.
- 70. Extended approaches: Paranasal sinuses are found to a relatively low- morbidity approach to selected tumors even inside the skull or brain. This can be divided into approaches to: anterior cranial fossa, mid cranial fossa, posterior cranial fossa, infratemporal fossa (incl. pterygopalatine fissure), sella turcica, orbital access, and optic nerve access. Complications: Proximity of the sinuses to the eyes, optic nerves, brain and internal carotid arteries Serious risks are rare occurrences
- 71. Before FESS 2 months after FESS
- 72. Principal element - granuloma formation - a conglomerate of macrophages, epithelioid cells, and multinucleated giant cells. 1. Infectious: spirochetes (syphilis, yaws) mycobacteria [tuberculosis, leprosy] bacterial [rhinoscleroma] fungus [aspergillus] 2. Inflammatory Wegener granulomatosis sarcoidosis, Churg-Strauss syndrome cocaine induced midline destructive lesions Granulomatous diseases
- 73. Cysts Mucocele and Pyocele Retention cyst Pseudocyst Post-operative maxillary cyst
- 74. Mucocele and pyocele Mucocele: formed when drainage of mucus from one of the paranasal sinuses becomes blocked by obstruction of its ostium. Contents: clear serous fluid, thick mucoid material, or, if hemorrhage has occurred, thick brown material Pyocele/mucopyocele: Infected mucocele Contents: mixture of mucus and pus from which a causative organism may or may not be seen on smear or subsequently cultured.
- 75. Pathogenesis: Blockage of the ostium pressure develops within sinus expansion of the sinus space erosion, and displacement of bone. Encroachment of the mucocele upon contiguous structure Sinus lining – remains normal or becomes attenuated to undergo metaplasia to low cuboidal or squamous cells.
- 76. Most commonly: frontal and anterior ethmoid sinuses Etiology: chronic inflammation, osteomas, fractures, tumors, polyps, scarring, and congenital abnormalities. Management Decompression by complete removal and curettage Marsupialisation via endoscopic approach through the middle meatus Prophylactic Nasofrontal duct obstruction
- 77. Retention cyst and Pseudocyst: Together called antral cyst or mucosal cyst Indistinguishable on radiological or clinical examination. Quite common. Mostly - single cysts, but in a few instances - they may be multiple and bilateral. Clinical features: Usually asymptomatic – discovered during radiographic examination Symptoms – similar to chronic sinusitis Sometimes an antral cyst may produce a swelling
- 78. Diagnosis :CT based Spherical, ovoid or dome-shaped radiopacities that have a smooth and uniform outline narrow or broad base. Size from minute to very large Usually remain static Many regress spontaneously
- 79. POST-OPERATIVE MAXILLARYCYST (SURGICALCILIATEDCYSTOFMAXILLA) Delayed complication arising years after surgery of maxillary sinus. Causes: Caldwell–Luc procedure including a nasal antrostomy Gun- shot injuries Fractures of the malar–maxillary complex Mid-face osteotomies. Clinical features: Pain, discomfort or swelling in the cheek or face, or intra-orally in the palate or alveolus. Pus discharge. Radiographs - well-defined radiolucent area closely related to the maxillary sinus. Treatment: enucleation.
- 80. TUMORS 0.2% of all malignancies 80% - maxillary sinus. Men>> women. 40 and 70 years. Carcinomas >> sarcomas Metastases are relatively rare. Tumours of the sphenoid and frontal sinuses are extremely rare - no standard staging system Most common - squamous cell carcinoma
- 81. WHO HISTOLOGICAL CLASSIFICATION OF NASAL AND PNS TUMORS
- 82. TNM CLASSIFICATION OF CARCINOMAS OF NOSE AND PARANASAL SINUSES .
- 83. Risk factors: 1. Woodworking (carpentry), Shoemaking, Metal-plating, Flour mill or bakery work. 2. Human papillomavirus (HPV) infection 3. Male 4. Older than 40 years. 5. Smoking.
- 84. Clinical features No signs or symptoms in the early stages. later: Blocked sinuses that do not clear, or sinus pressure. Headaches or pain in the sinus areas. Rhinitis and epistaxis A lump or sore inside the nose that does not heal. A lump on the face or roof of the mouth. Numbness or tingling in the face. Swelling or other trouble with the eyes, such as double vision or the eyes pointing in different directions. Pain in the upper teeth, loose teeth, or dentures that no longer fit well. Pain or pressure in the ear.
- 85. Treatment 1. Surgery: For all stages of paranasal sinus and nasal cavity cancer. Transfacial approaches 1. lateral rhinotomy/ weberfergussen incision 2. diffenbech extension 3. Lynch extension with the modification External ethmoidectomy/frontoehtmoidectomy Bicoronal with Mid face degloving Subcranial approach Acess osteotomies
- 86. Trans oral approach: Caldwell lue Denker Janson – horgan approach Trans nasal: Transseptal approach Endoscopic approaches
- 87. Draw backs of endoscopic approach -Not indicated in case of extensive involvement Trans orbital extension Scar tissue due to previous surgery in case to reduce the bony fracture
- 88. TRANSORAL ROBOTIC SURGERY New advances in technology facilitate minimal access To avoid large transcervical or face-splitting incisions. Transoral robotic surgery allows access to tumors within the posterior oral cavity and oropharynx via multiple robotic arms and a high-definition/ magnification camera. The operator sits at a separate console and via remote control can operate the various instruments. Electrocautery, laser, and standard dissection instruments can be used with the robot. Advantages include surgical access via minimal approaches, resulting in definitive pathologic assessment while minimizing transection and resection of critical swallowing musculature Oral Maxillofacial Surg Clin N Am 24 (2012) 307–316
- 89. Trans oral Robotic surgery more-precise movements in narrow spaces and the capability to work around corners. This result in preservation of maximum amount of healthy muscular and neurovascular tissue which helps the patient swallow on their own sooner and discharged home earlier.
- 90. 1. Radiation therapy: External radiation therapy, Internal radiation therapy - depending on the type and stage of the cancer being treated. IMRT: Intensity-modulated radiation therapy (IMRT) can deliver high doses of radiation with precision while minimizing damage to surrounding tissues. IMRT can conform to the irregular shape of a tumor, delivering higher doses directly to the tumor cells and potentially destroying more tumor cells. The technique requires more precise planning due to the sharp dose falloff gradient between the gross tumor and the surrounding normal tissue. IMRT provides locoregional control (90%) and is well tolerated by patients. Oral Maxillofacial Surg Clin N Am 24 (2012) 307–316
- 91. Chemotherapy: Systemic chemotherapy: When chemotherapy drug is given PO, IV or IM the drugs enter the bloodstream and can reach cancer cells throughout the body Regional chemotherapy: When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity, the drugs mainly affect cancer cells in those areas. Combination chemotherapy is treatment using more than one anticancer drug. The way the chemotherapy is given depends on the type and stage of the cancer being treated. Intra arterial cisplastin therapy: As a primary therapy, the complete response rate was 83.3%, The 2-year local control rate was 63.0%, and the 2-year overall survival rate was 75.5%. The 2-year preservation rate of the hard palate was 97.1%, that of the eyeball was 97.2%, and that of visual function was 94.4%. This treatment regimen can contribute to improving the quality of life of patients without reducing the curability of the therapy. Int. J. Oral Maxillofac. Surg. 2015; 44: 697–704.
- 92. Other surgically relevant conditions Oro-antral communication/fistula Antral foreign bodies Hypertrophied maxillary sinus
- 93. Oro-Antral Fistula (oaf) Oro-antral communication: it is an abnormal connection between oral and Antral cavities. Oro-antral fistula: long standing oro-antral communication when left open, epithelializes to form a patent fistula between the two cavities. Types: ALVEOLOSINUSAL PALATO-SINUSAL VESTIBULO-SINUSAL Oro-Antral Communications
- 94. CAUSES: Extraction – maxillary posterior teeth Cysts, tumors Osteomyelitis Radiation therapy Trauma Implant denture CLINICAL FEATURES: Some patients are asymptomatic Unpleasant tasting discharge and odor Reflux of fluids and foods into the nose from mouth Leakage of air Difficulty in smoking and blowing air Development of chronic sinusitis in infected cases
- 95. Diagnosis: Valsalva maneauver Mirror fog test Cotton wisp test Nasal regurgitation of fluid Radiographs: Sinus floor discontinuity, Sinus opacity, Focal alveolar atrophy, Associated periodontal disease Oro-Antral Communications (UL7)
- 96. Treatment: Immediate treatment: Primary purpose is closure of defect and prevention of sinusitis through: Suturing across the defect with/without periodontal pack, warm saline rinses, antibiotic and antihistaminic therapy with decongestants. Size < 5mm: non-invasive intervention (spontaneous closure by blood clot) Size > 5mm, and > 48 hours - : surgical closure : small defects – local flaps; large defects – regional/distant flaps.
- 97. Obturators Buccal Advancement Flap most common. Described by Rehrmann & made popular by Berger. Trapezoidal sliding flap – Moczair buccal osteoperiosteal flapOro-Antral Communications
- 98. Palatal flaps 1. Palatal rotational advancement flap most common 2. V-shaped palatal flap (kruger) & 3. Split-thickness palatal flap (ito & hara).Oro-Antral Communications
- 99. Combination flaps Inverted periosteal flap Tongue flap, temporalis flap BFP closure PRF membrane coverage Autologous bone grafts: press-fit technique Autologous cartilage grafts: auricular cartilage, auricular cartilage Alloplastic materials Transplantation of a mature wisdom tooth (followed by root canal treatment of the tooth 5 - 6 weeks later) Laser bio-stimulation (over 5 days) Oro-Antral Communication
- 100. ANTRAL FOREIGN BODIES: Gutta-percha points, tooth roots, impression materials, dental burs, bone pieces , implants etc.. Treatment has been direct explored by Caldwell-Luc approach, with or without nasal antrostomy. FESS may be done for sinusitis. HYPERTROPHIED MAXILLARY SINUS: Not pathology but causes difficulty in implant supported rehabilitation of posterior maxilla, with the risk of subsequent development of sinus pathologies. The management includes direct and indirect sinus lifting. Oro-Antral Communications (UL8)
- 101. Complications Because of the proximity of the paranasal sinuses to the eyes and brain, complications of sinusitis are divided into orbital, neurological and local complications.
- 102. Orbital complications highest frequency - in children under 6 years of age. Infection usually originates from the ethmoids and occurs through: (1) direct extension through the orbital wall (2) retrograde spread through veins between the sinuses and the orbit. Lymphatic spread – not significant
- 103. Orbital complications 1. Preseptal cellulitis, or periorbital cellulitis 2. Orbital cellulitis and edema 3. Subperiosteal abscess 4. orbital abscess 5. Cavernous sinus thrombosis: direct extension or retrograde thrombophlebitis (via the ophthalmic vein) of ethmoid or sphenoid infections. restriction of extra ocular mobility, proptosis, chemosis, and visual loss cranial neuropathies and signs of meningitis
- 104. Neurological complications Less frequently than orbital Most commonly related to the frontal or sphenoid sinuses. Via - direct spread or retrograde thrombophlebitis. A – osteomyelitis B - periorbital abscess C – epidural abscess D – subdural abscess E – brain abscess F – meningitis G - septic thrombosis of superior sagittal sinus
- 105. Local complications Osteomyelitis - complication of frontal sinusitis. Tender, doughy, erythematous swelling over the forehead. Treatment of choice - surgical eradication of the affected bone under antibiotic coverage.
- 106. REFERENCES 1. References: 2. Peterson’s principles of oral and maxillofacial surgery DISEASES of the SINUSES Diagnosis and Management- DAVIDW. KENNEDY, MD, FACS 1. WHO classification of head and neck tumors 2. PL Dhingra - Disease of ear, nose & throat 4th edition 3. Rosai and Ackerman’s Surgical Pathology (9th edition) 4. David L. Daniels et.al. The Frontal Sinus Drainage Pathway and Related Structures, AJNR: 24, August 2003. 5. Interactive Atlas. http://uwmsk.org/sinusanatomy2/axial/axial.html 6. (Adapted from Chow AW, Benninger MS, Brook I, et al: IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clinical Infectious Diseases 54 (8):1041–5 (2012).) 7. Thompson and Patterson: Fungal disease of the nose and paranasal sinuses:J Allergy Clin Immunol 2012;129:321-6. 8. Multiplanar Sinus CT: A Systematic Approach to Imaging Before Functional Endoscopic Sinus Surgery Jenny K. Hoang, James D. Eastwood, Christopher L. Tebbit, and Christine M. Glastonbury American Journal of Roentgenology 2010 194:6, W527-W536
- 107. Raef S. Ahmed, Roger Ove, Jun Duan, Richard Popple, Glenn B. Cobb Intensity-modulated radiotherapy (IMRT) for carcinoma of the maxillary sinus: A comparison of IMRT planning systems Medical Dosimetry, Volume 31, Issue 3, Autumn 2006, Pages 224-232 Management of rhinomaxillary mucormycosis with Posaconazole in immunocompetent patients Sachin Rai *, Shikha Yadav, Dinesh Kumar, Vijay Kumar, Vidya Rattan Journal of Oral Biology and Craniofacial Research xxx (2016) xxx Modified transnanal endoscopic maxillectomy: a novel surgery style of maxillary malignant tumor Yonghua Bi1,2, Shuangba He1, Tao Guo1, Jingwu Sun Int J Clin Exp Med 2016;9(6):11361-11366 Modified double-layered flap technique for closure of anoroantral fistula: Surgical procedure and case reportAlberto Merlinia, Joseph Garibaldia, Matteo Piazzaia, Luca Giorgisb, British Journal of Oral and Maxillofacial Surgery 54 (2016) 959–961 Repair of Oroantral Communication by Use of a Combined Surgical Approach Functional Endoscopic Surgery and Buccal Advancement Flap/Buccal Fat Pad Graft Timothy Adams, DDS,* Daniel Taub, DDS, MD,y and Marc Rosen, MD. J Oral Maxillofac Surg 73:1452-1456, 2015 An Update on Squamous Carcinoma of the Oral Cavity,Oropharynx, and Maxillary SinusJoshua E. Lubek, DDS, MDa,*, Lewis Clayman, DMD, MD Oral Maxillofacial Surg Clin N Am 24 (2012) 307–316
- 108. Thank you