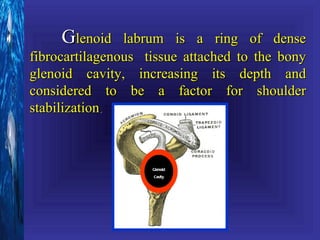
1. The document discusses various shoulder joint diseases including rotator cuff disorders, instability, biceps disorders, tumors, arthritis, and referred pain.
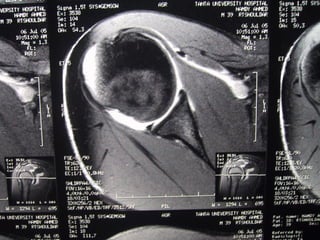
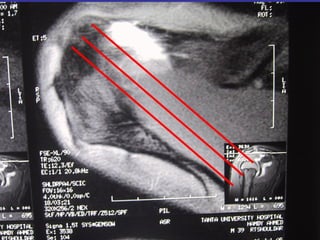
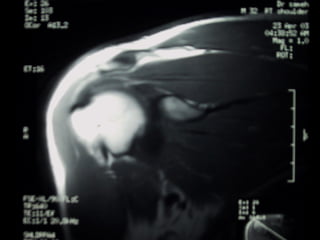
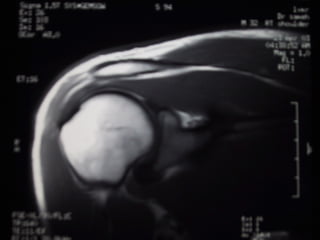
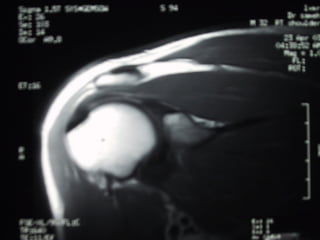
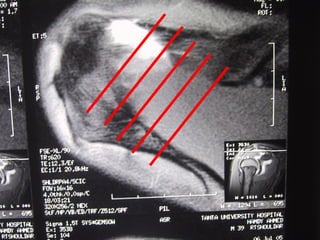
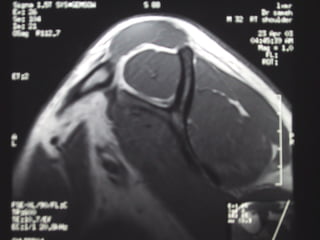
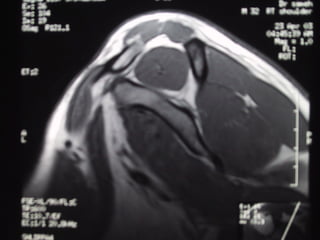
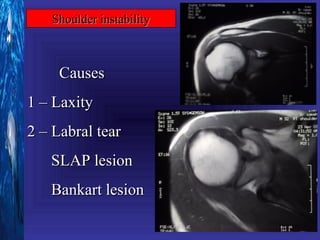
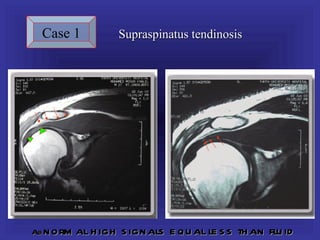
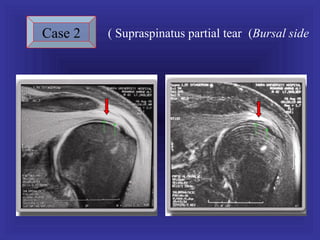
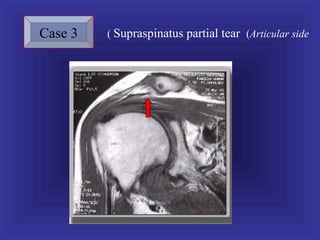
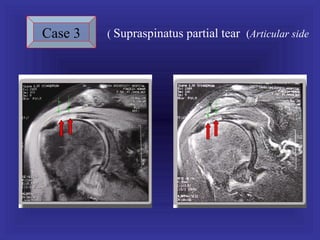
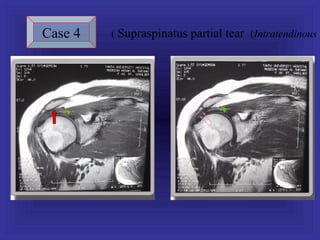
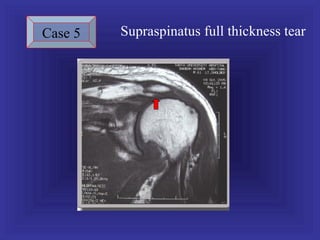
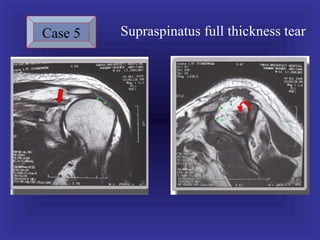
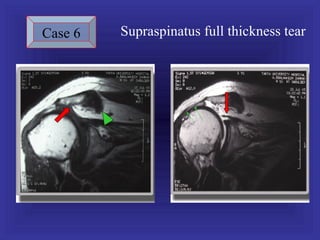
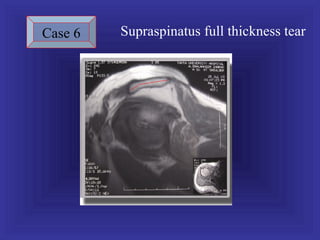
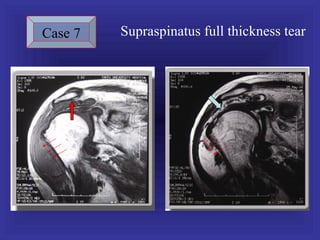
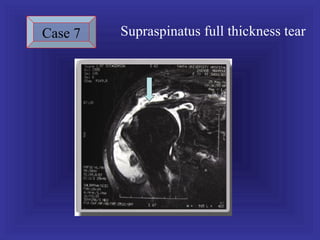
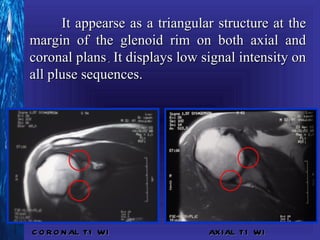
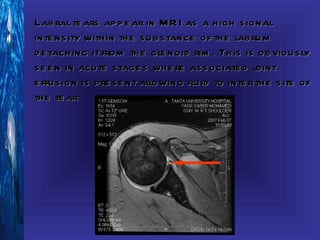
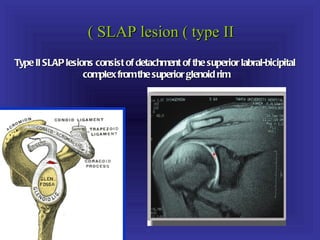
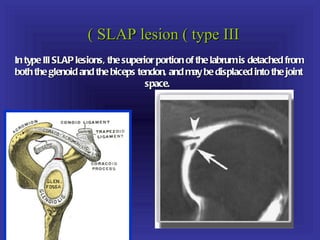
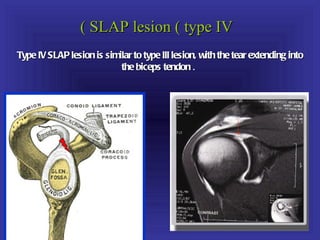
2. Rotator cuff tears are classified as partial-thickness or full-thickness and can be caused by impingement or trauma. Glenoid labral tears appear on MRI as high signal intensity detachment from the glenoid rim.
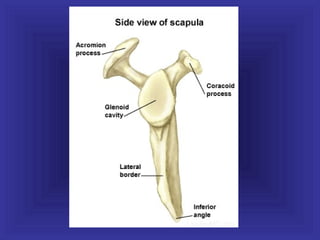
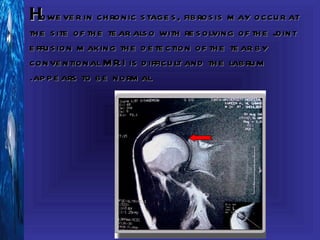
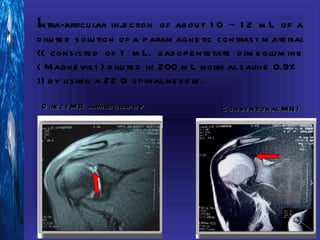
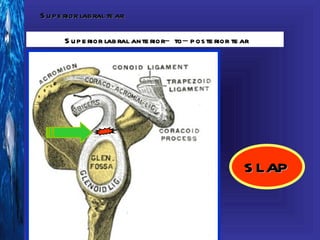
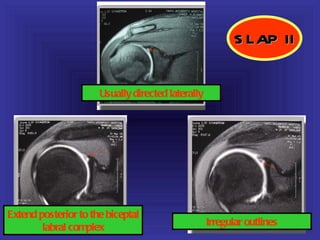
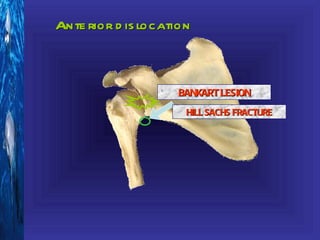
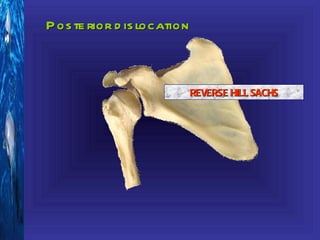
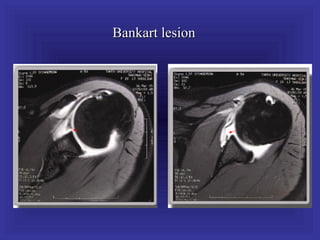
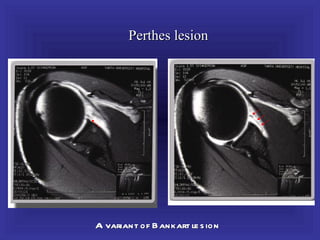
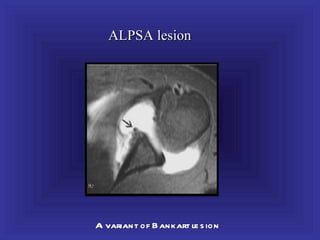
3. Direct MR arthrography improves detection of chronic labral tears by distending the joint with contrast. Common labral tears include SLAP lesions, Bankart lesions, and Hill-Sachs fractures associated with instability.