Downloaded 80 times

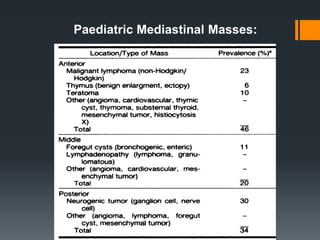
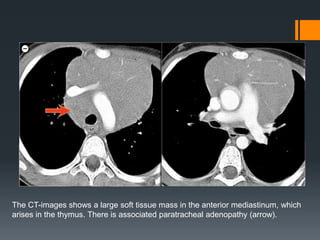

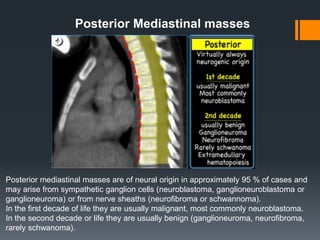

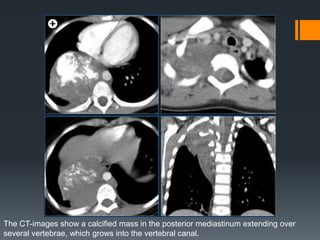

The document discusses various pediatric mediastinal masses including lymphoma, thymic lesions, germ cell tumors, and neurogenic tumors. Lymphoma is one of the most common mediastinal neoplasms in children and can manifest as Hodgkin's or non-Hodgkin's disease. Other masses discussed include thymic hyperplasia, thymoma, cysts, and teratomas. Posterior mediastinal masses are often neural in origin and may be malignant neuroblastomas or benign ganglioneuromas. CT and MRI are useful in characterizing the appearance and extent of these pediatric mediastinal masses.











































































































