Downloaded 364 times


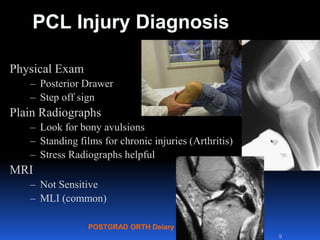


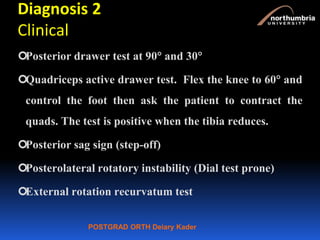
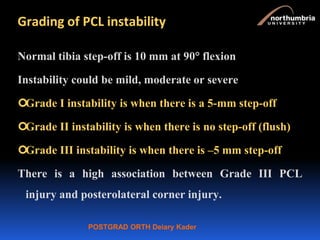
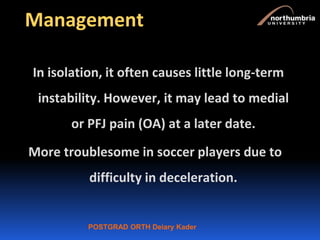
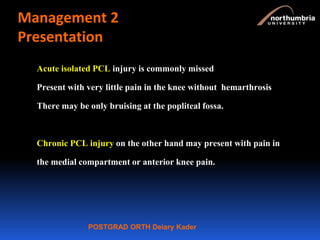

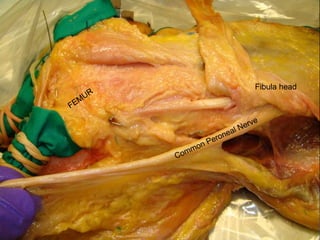

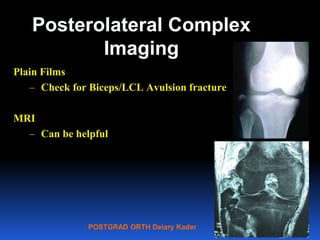
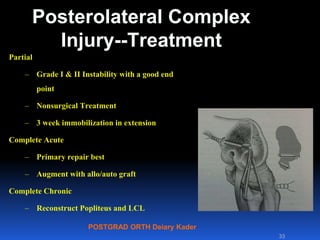
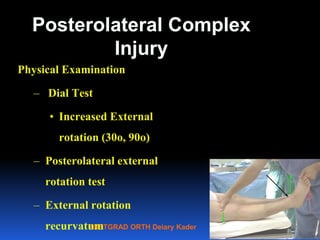
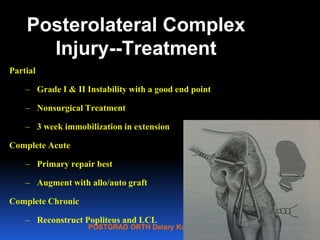
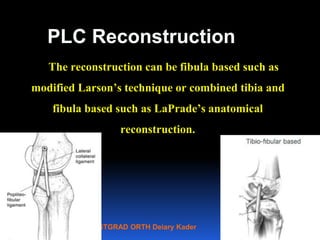
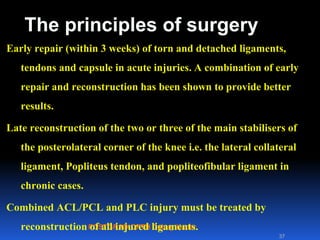
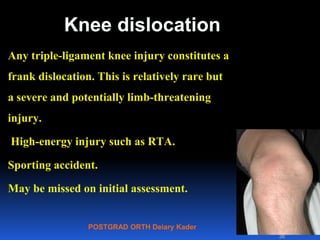
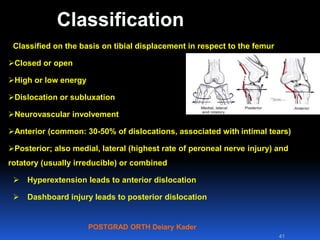

This document contains lecture slides from Professor Deiary Kader on various topics related to orthopaedics of the knee. It discusses the anatomy and classification of knee stabilizers. It provides details on the posterior cruciate ligament anatomy, mechanisms of injury, grading of instability, and treatment options including rehabilitation and reconstruction. The document also discusses the posterolateral corner complex, its anatomy, mechanisms of injury, examination techniques, and treatment including non-surgical and surgical options. Finally, it covers knee dislocations, classification, examination, management principles, and surgical approaches.




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













