Downloaded 68 times





















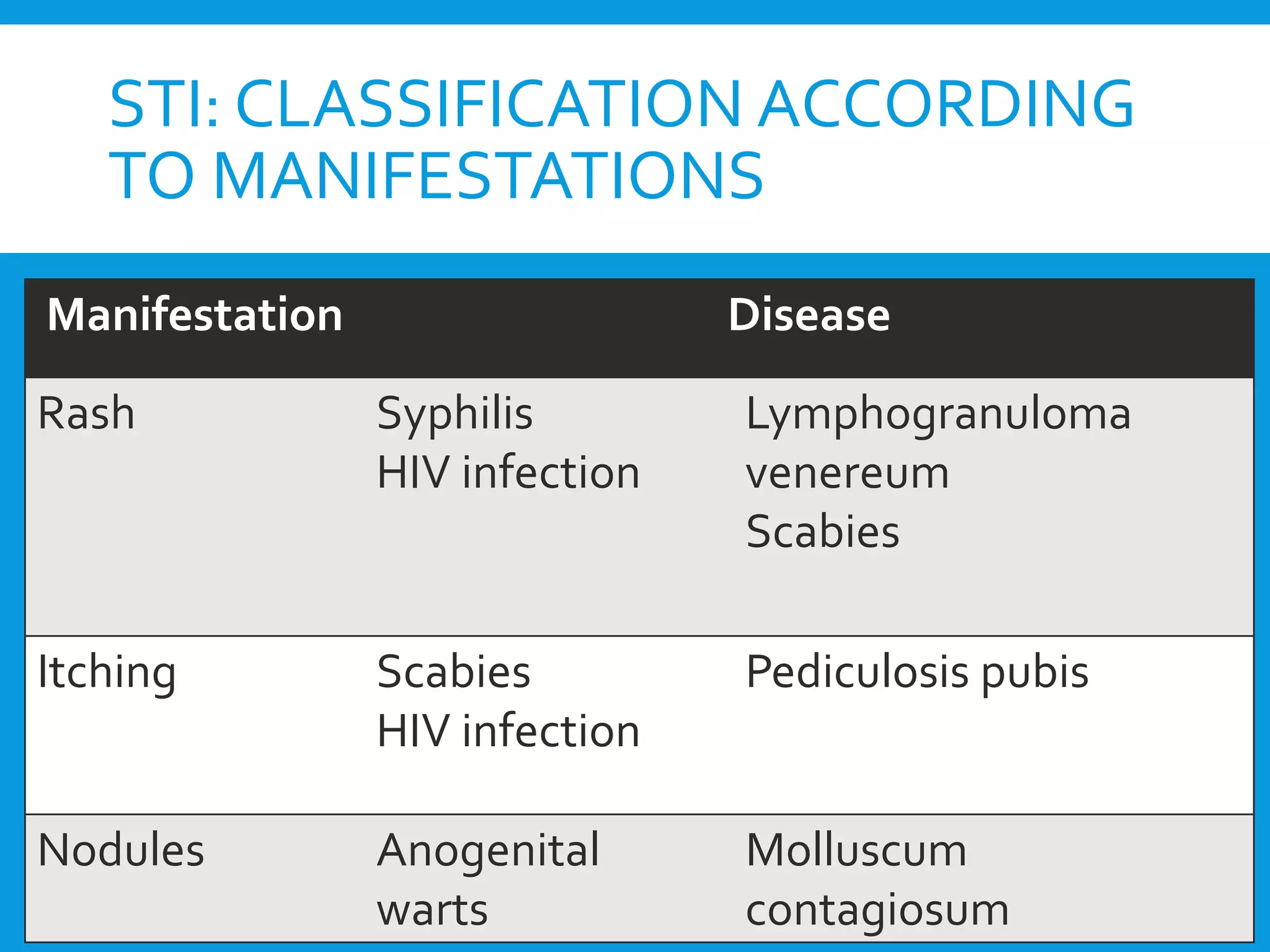





The document discusses drugs used to treat sexually transmitted infections. It begins by defining key terms like venereal disease, sexually transmitted disease, and sexually transmitted infection. It then covers the etiological classification of STIs, listing the causative organisms for various conditions. The majority of the document discusses treatment for specific STIs, including drugs, doses, and regimens used to treat infections like syphilis, gonorrhea, chlamydia, herpes, and HIV/AIDS. It also covers the syndromic approach for STI treatment, which classifies infections according to clinical manifestations and recommends therapy using clinical algorithms.























































































