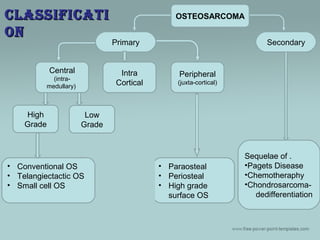
Osteosarcoma is a malignant bone tumor that arises from primitive bone-forming cells. It most commonly occurs in adolescents and young adults. The most frequent sites are the distal femur, proximal tibia, and proximal humerus. Treatment involves preoperative chemotherapy, surgical resection with wide margins, and postoperative chemotherapy. Prognosis depends on the stage, with 5-year survival rates of 60-80% for localized tumors and 15-30% for those that have metastasized.






![SKELETAL DISTRIBUTIONSKELETAL DISTRIBUTION
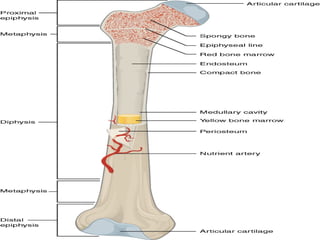
• Sites
– Metaphysis > Diaphysis > Epiphysis
[89%] [10%] [1%]
• Distal Femur [40%]
• Proximal Tibia [20%]
• Proximal Humerus [10%]
• Others – Jaw [8%] or
Pelvis [8%]](https://image.slidesharecdn.com/osteosarcoma-150602132720-lva1-app6892/85/Osteosarcoma-10-320.jpg)