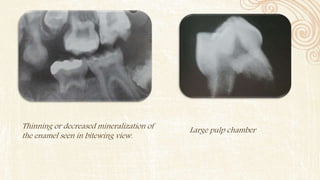
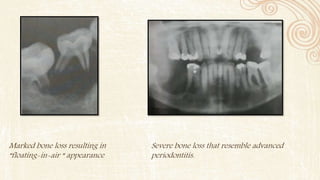
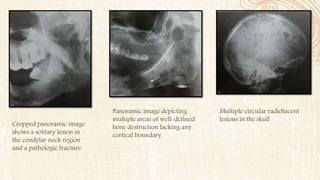
This document discusses several diseases that can affect bone density and structure, including hyperparathyroidism, osteoporosis, osteomalacia, leukemia, Langerhans cell disease, Paget's disease, and multiple myeloma. It provides details on the clinical features, radiographic manifestations, differential diagnosis, and management of each condition. The document contains radiographic images showing examples of bone changes associated with some of the diseases.