Downloaded 80 times


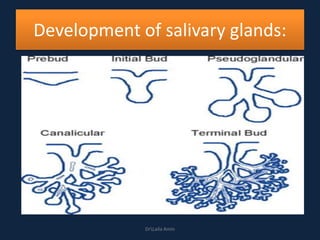

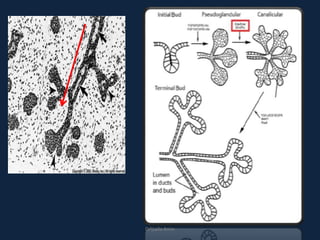
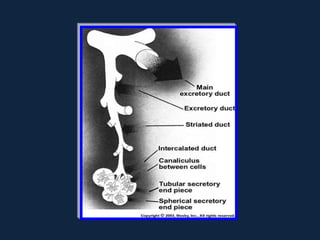
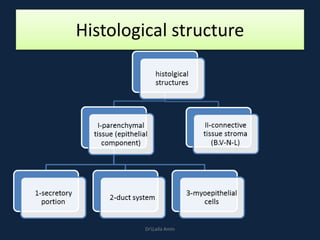
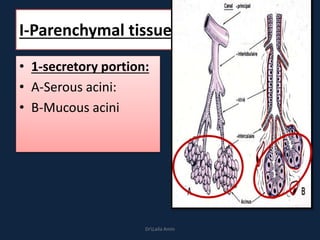
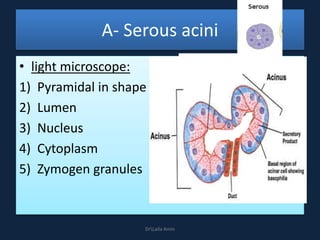
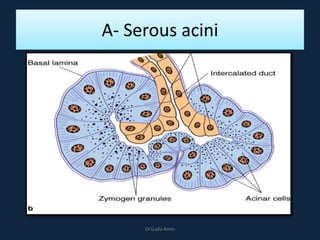
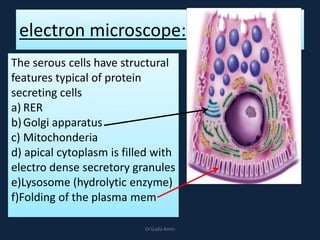

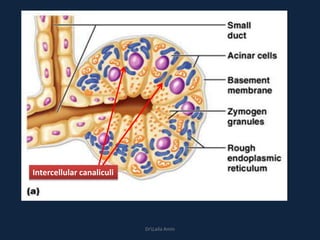
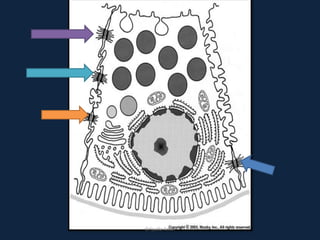

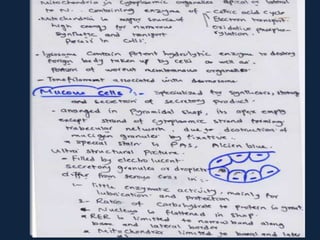
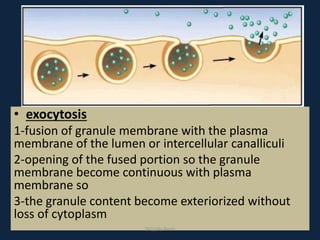
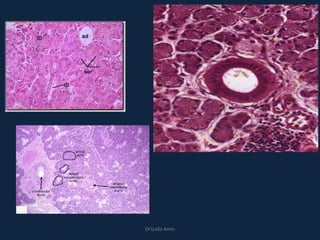
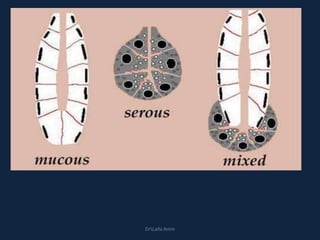
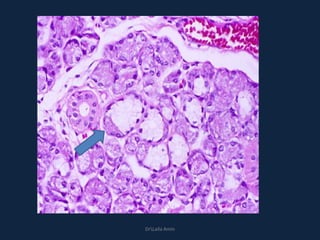
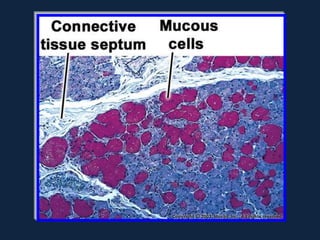
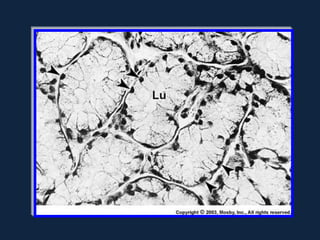
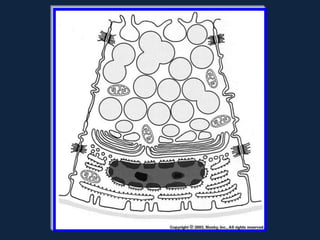
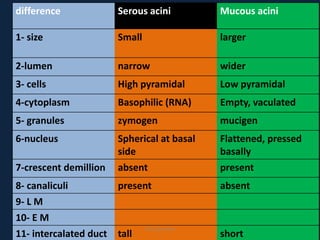
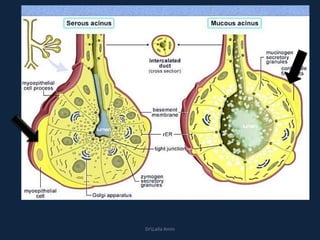

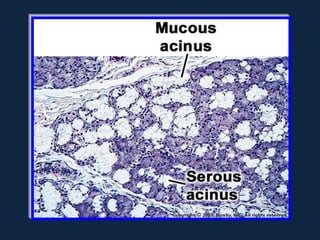
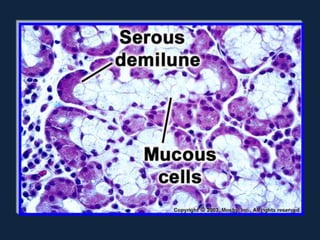
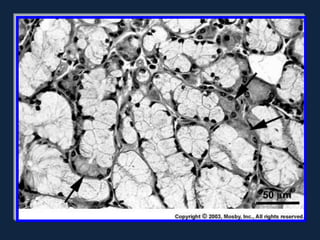

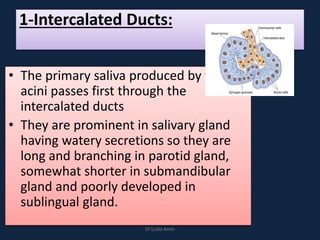

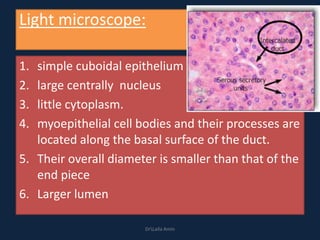
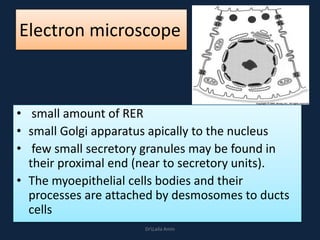
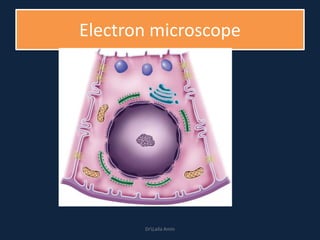


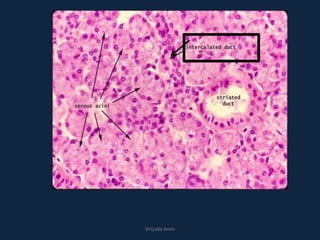



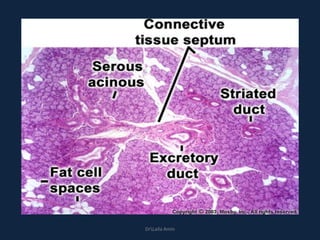



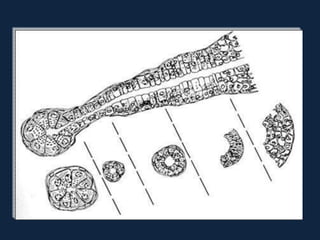
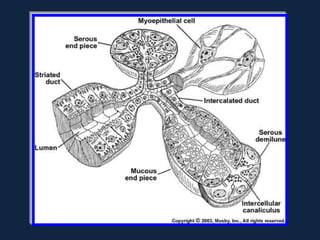
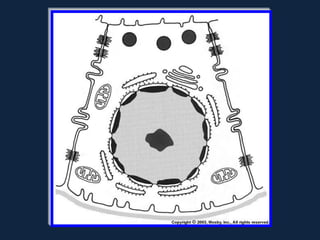
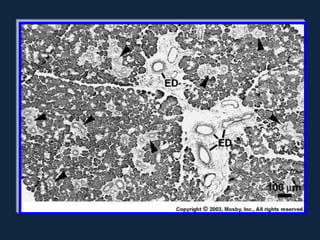
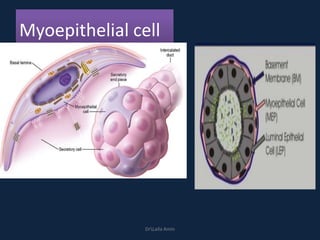
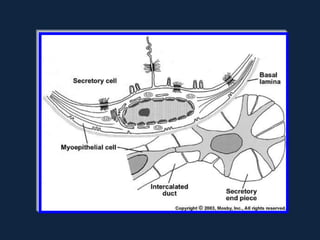
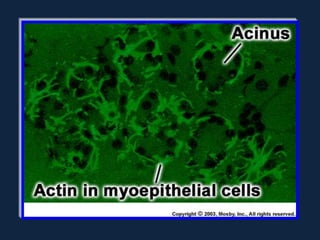



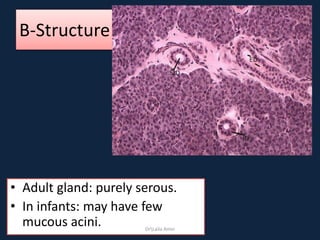

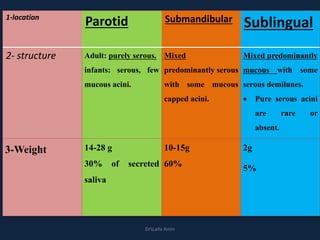
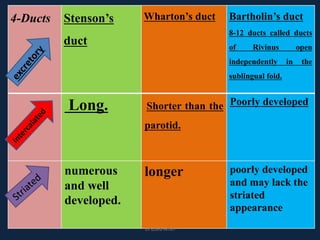
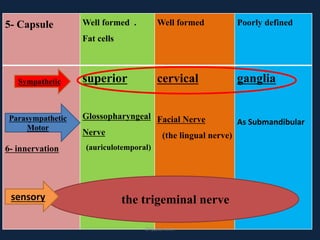
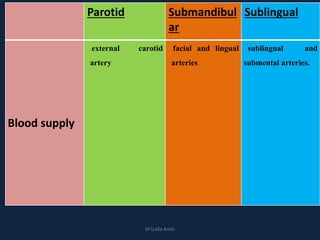
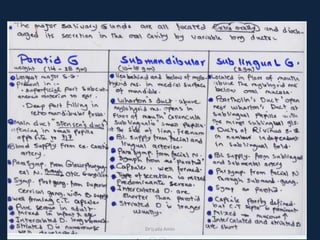
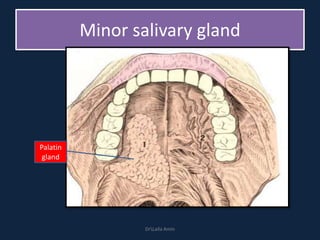

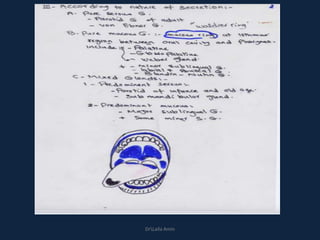
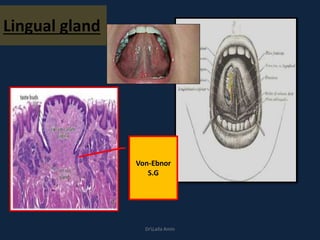







The document discusses the development and histological structure of salivary glands. It begins by describing how salivary glands arise from an epithelial outgrowth from the oral epithelium that branches and canalizes to form the duct system. It then details the microscopic structure of the different cell types found in salivary glands, including serous and mucous acinar cells, and the intercalated, striated, and excretory ducts. Specifically, it focuses on the cellular features, organelles, and secretory mechanisms of each cell type. Finally, it briefly discusses the connective tissue capsule and septa that encapsulate the glands.



























































![]Dental Occlusion part 1](https://cdn.slidesharecdn.com/ss_thumbnails/occlusionpart1-160420073612-thumbnail.jpg?width=640&height=640&fit=bounds)
























