Downloaded 160 times































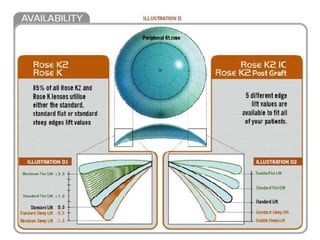
















Here are 3 options for very difficult post-graft cases when standard lenses are not working: 1. Try a scleral lens with a large optic zone to vault over the irregularity. This can improve comfort and vision. 2. Consider corneal collagen cross-linking (CXL) to strengthen the cornea followed by intracorneal ring segments (Intacs) to help regularize the shape. 3. As a last resort, a second corneal transplant may be needed to obtain an adequate surface for contact lens wear or improve vision. However, the success rate decreases with subsequent grafts. The key is finding the best option to improve vision and comfort while protecting the ocular surface long-term. A
![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)










































































































