Downloaded 198 times

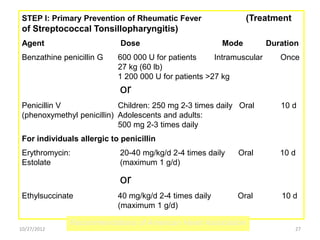
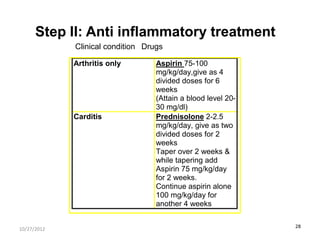

The document discusses rheumatic fever, a disease that can occur after a streptococcal throat infection and causes inflammation in connective tissues, especially the heart. It causes symptoms like arthritis, heart issues, involuntary movements, and skin rashes. The document covers the causes, symptoms, diagnosis, treatment, and prevention of rheumatic fever through antibiotics and lifestyle changes.




































































