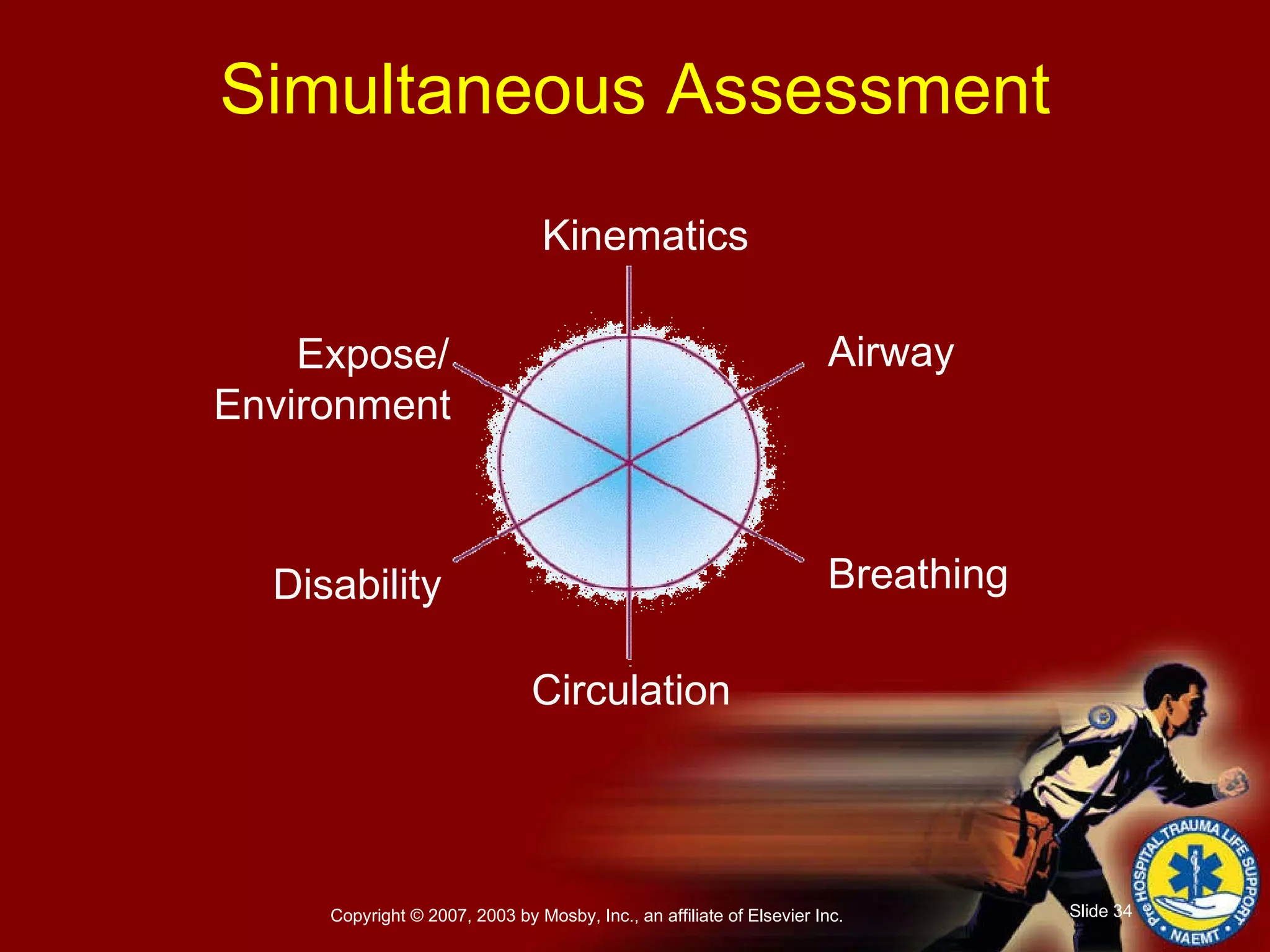
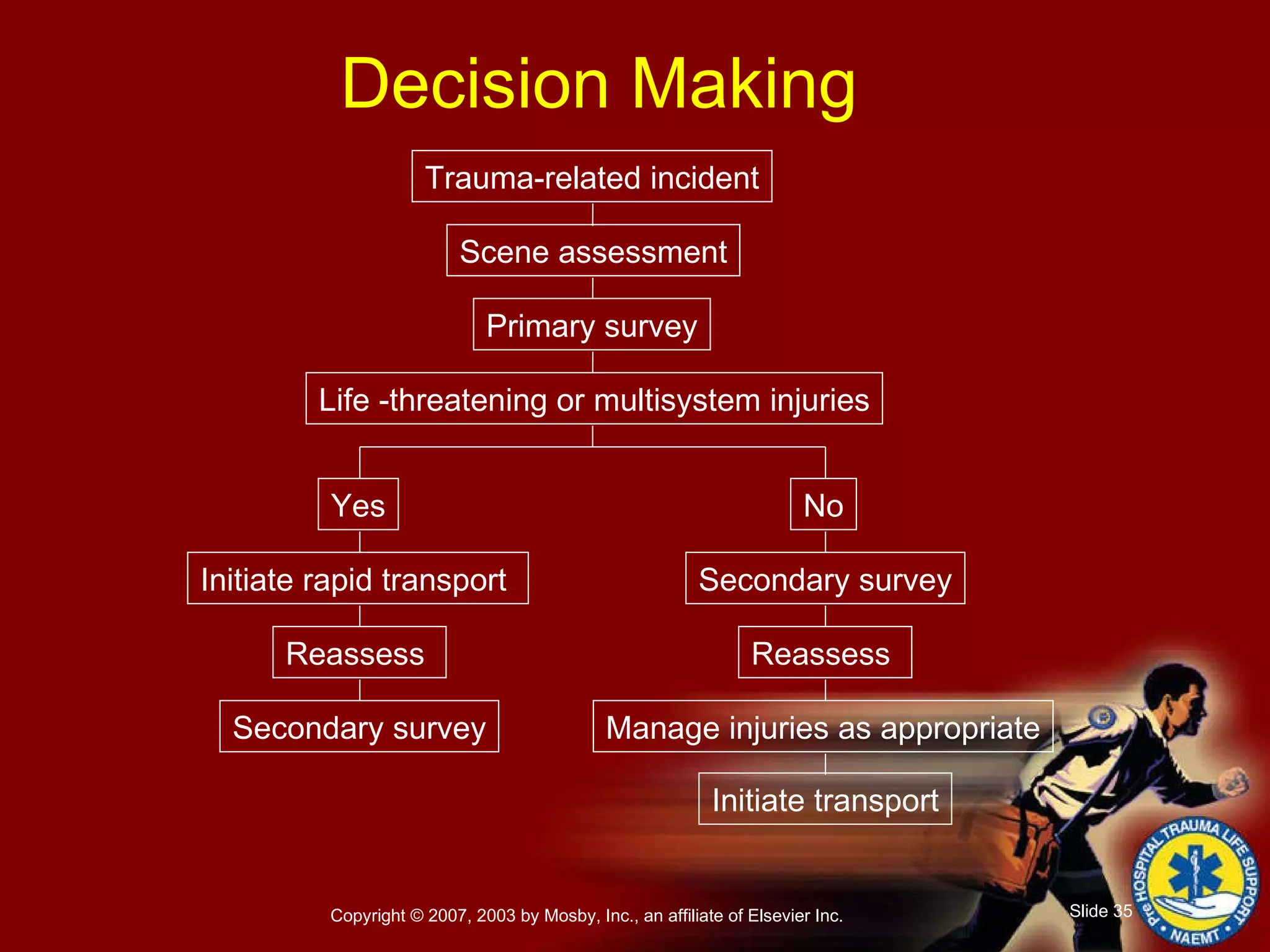
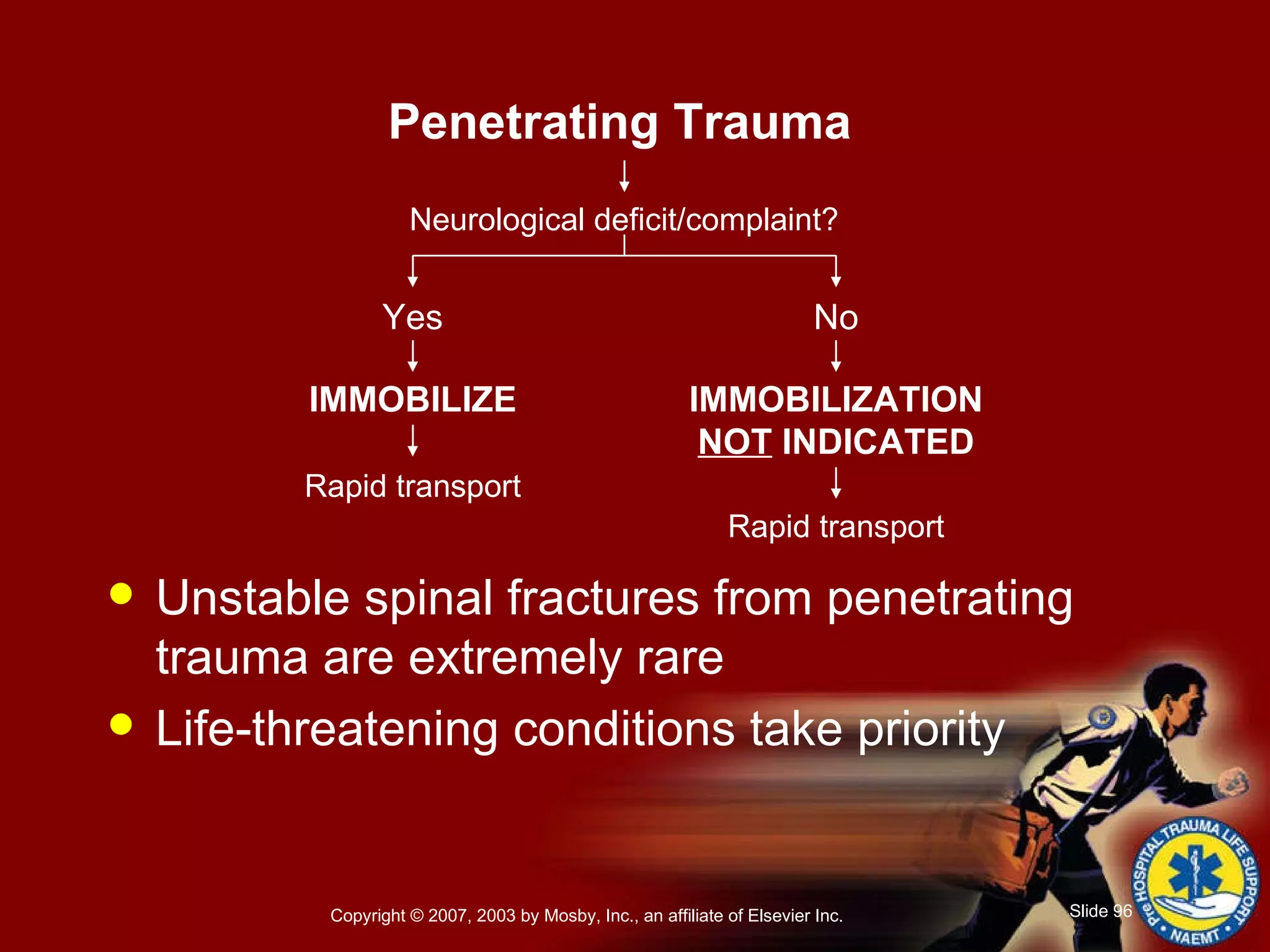
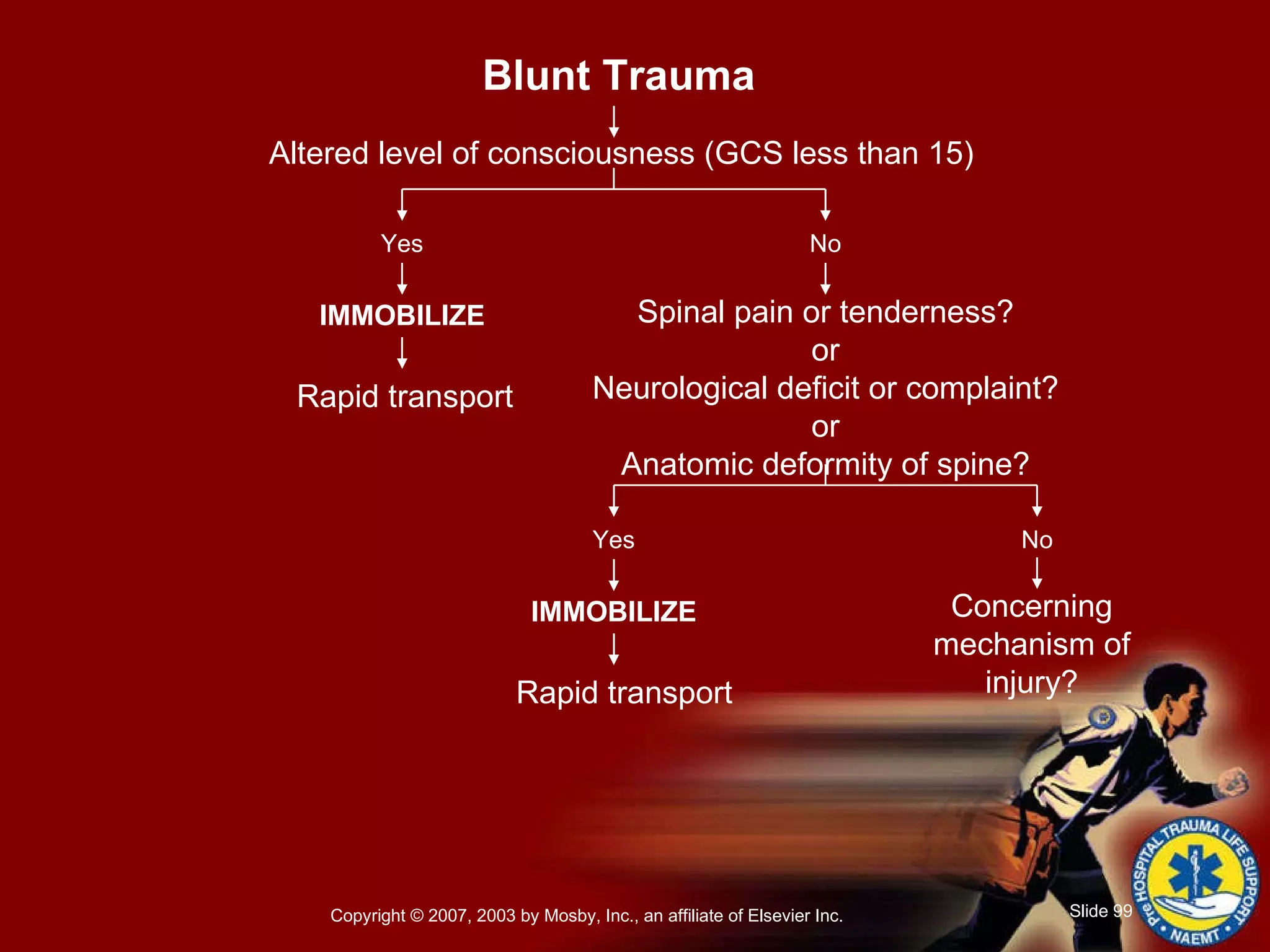
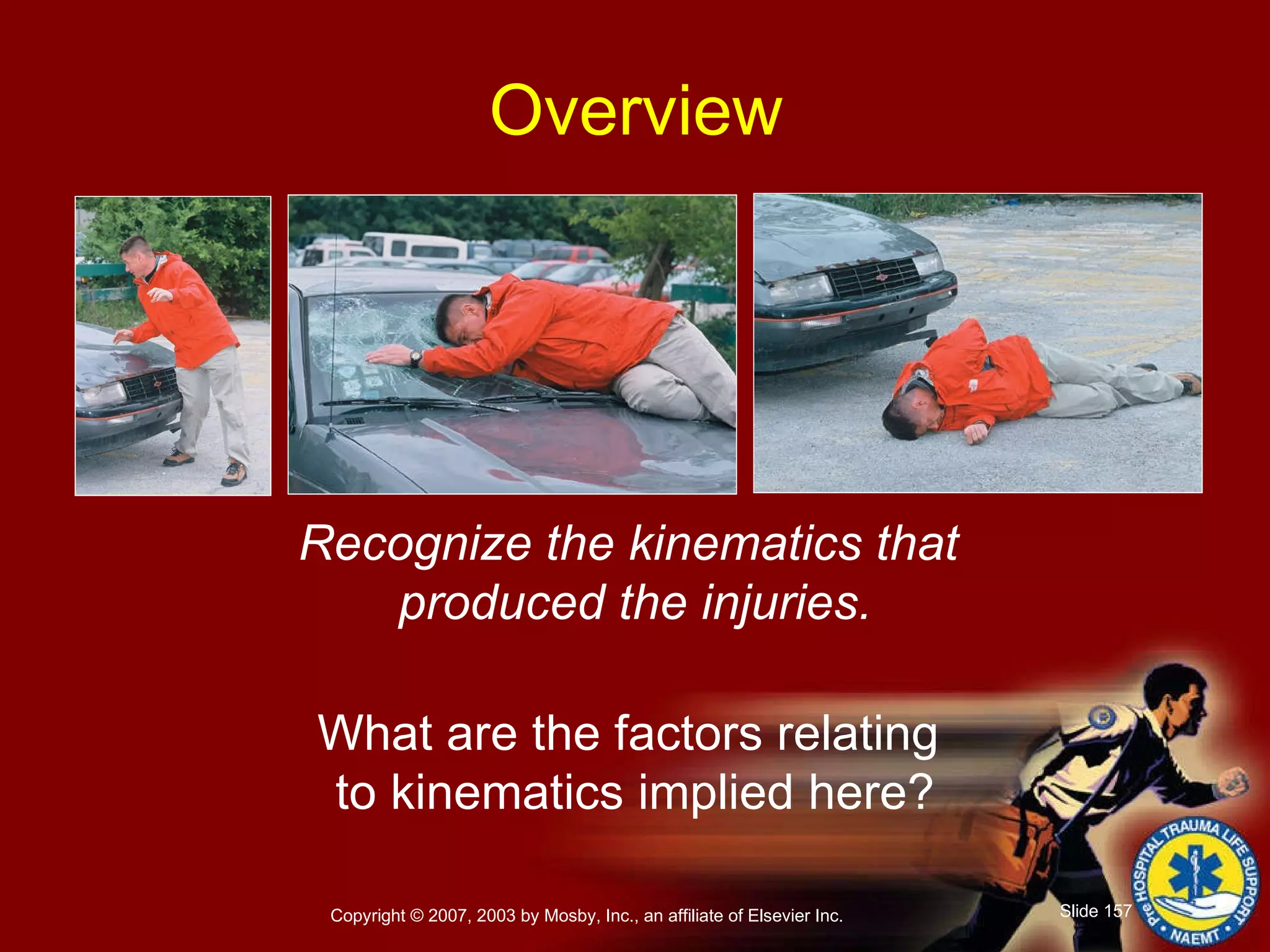
The document provides an overview of a prehospital trauma life support refresher course. It discusses topics like the kinematics of different types of injuries, management of shock, airway management techniques, spinal immobilization, and assessment and management of head, chest, abdominal and spinal trauma. Key skills like the primary and secondary survey process are also reviewed.