Downloaded 2,083 times
![• Prolonged use of local or systemic
corticosteroids:- Long-term use of topical and
systemic steroids produces secondary open-
angle glaucoma similar
to chronic simple glaucoma. The increased
intraocular pressure
[IOP] caused by prolonged steroid therapy is
reversible but the damage produced by it is
irreversible. (edema glucocorticoid receptors
on trabecular meshwork cells.)](https://image.slidesharecdn.com/glaucoma-181026045423/85/Glaucoma-11-320.jpg)
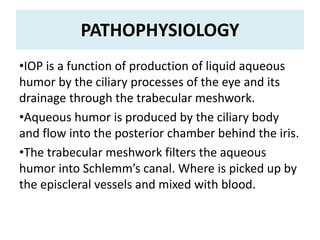
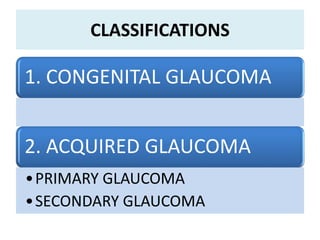
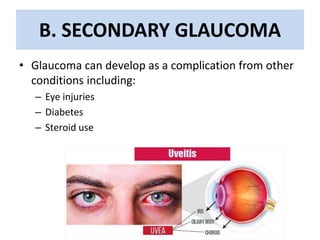
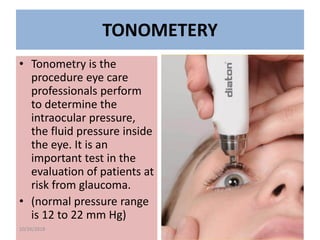

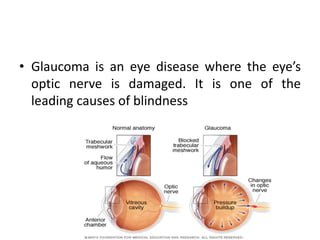
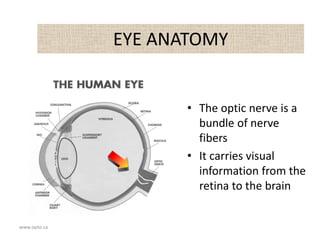
Glaucoma is a group of eye disorders characterized by high intraocular pressure (IOP), leading to optic nerve damage and potential blindness if untreated. Risk factors include genetics, aging, eye trauma, and certain medical conditions, while types of glaucoma include congenital and acquired forms, with primary open-angle glaucoma being the most common. Diagnosis involves thorough eye examinations and various tests, with management focusing on medication and surgical options to lower IOP and preserve vision.