This document contains summaries of ECG findings for various patients. Key cases include:
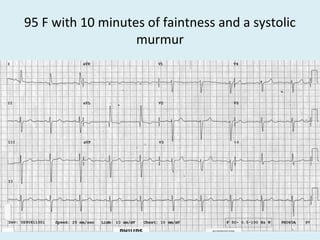
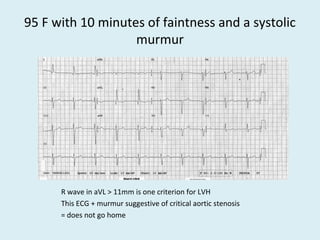
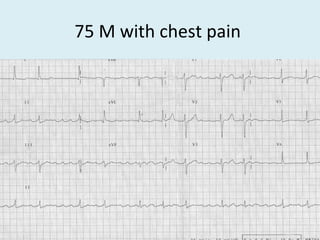
- A 95-year-old patient with faintness and a systolic murmur, whose ECG and murmur were suggestive of critical aortic stenosis.
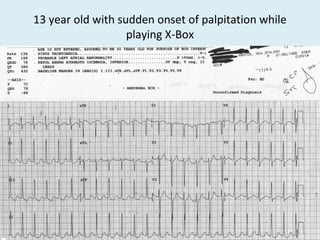
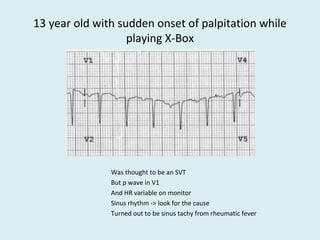
- A 13-year-old with sudden palpitations found to have sinus tachycardia from rheumatic fever.
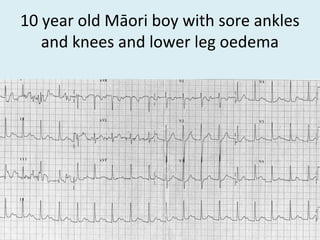
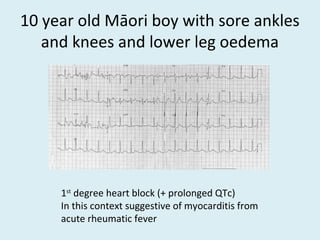
- A 10-year-old Māori boy with joint pain and swelling found to have myocarditis from acute rheumatic fever, shown on his ECG.
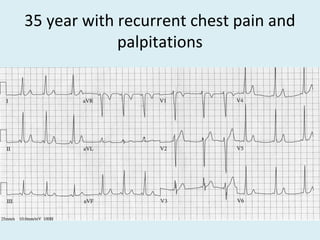
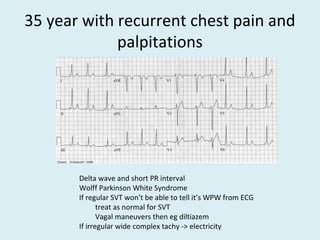
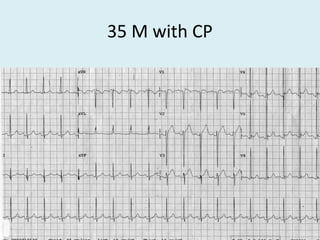
- A 35-year-old with chest pain and palpitations found to have Wolff-Parkinson-White syndrome.
The document




















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












