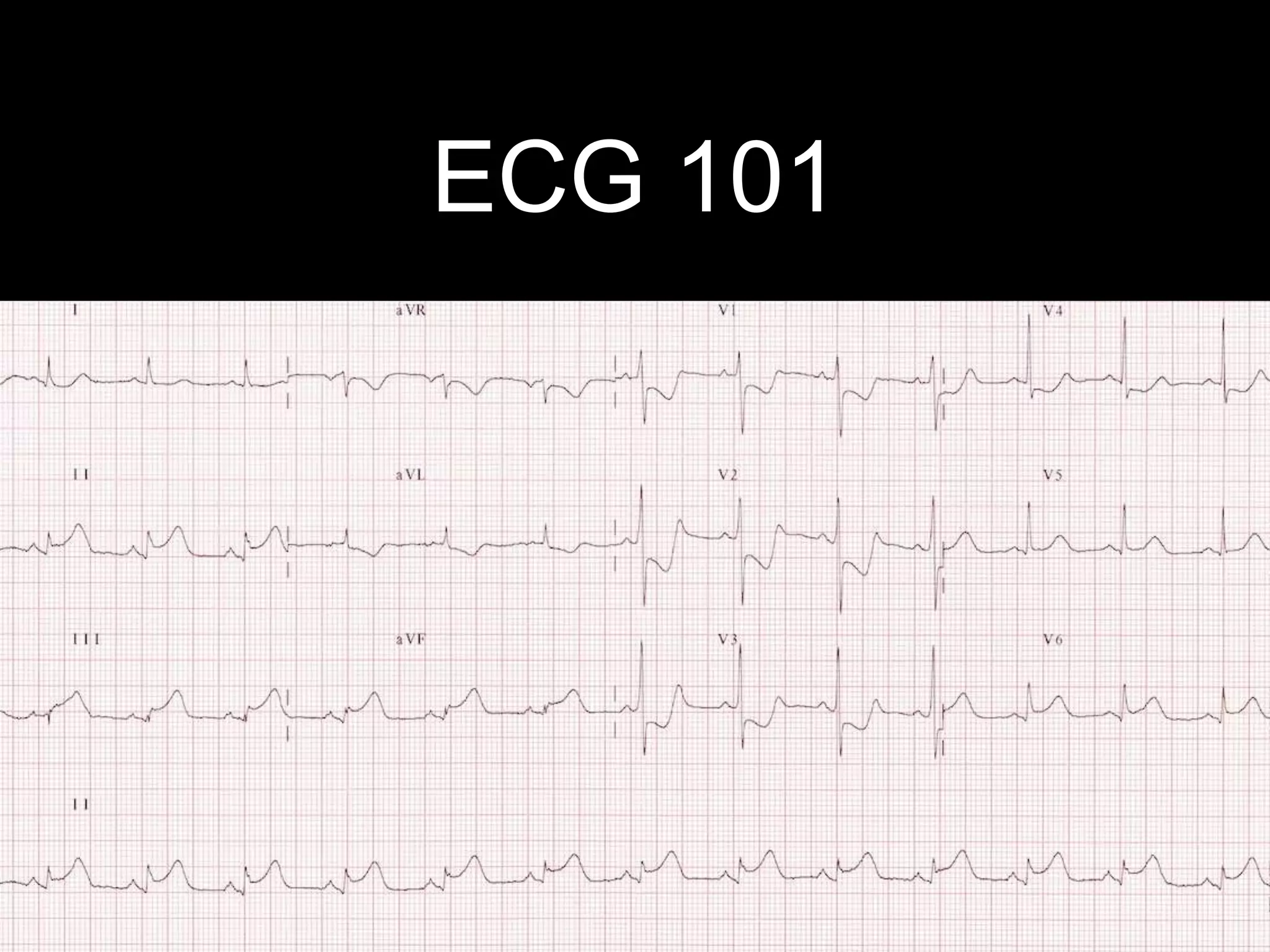
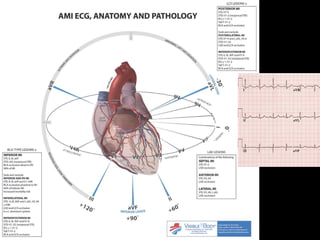
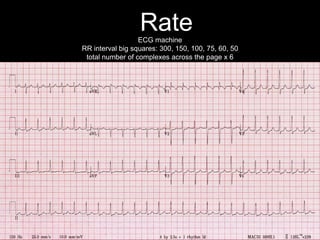
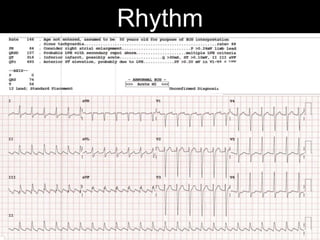
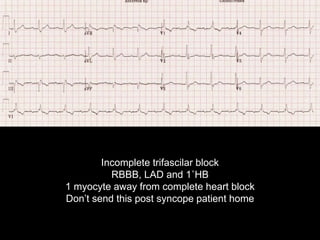
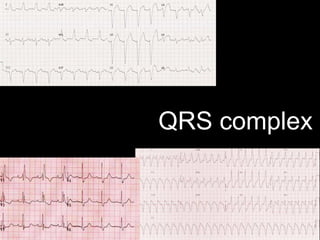
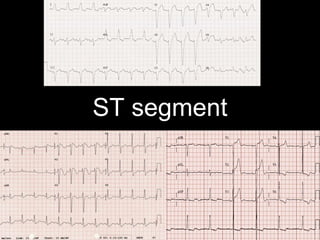
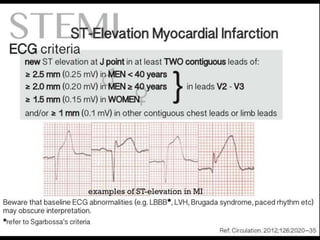
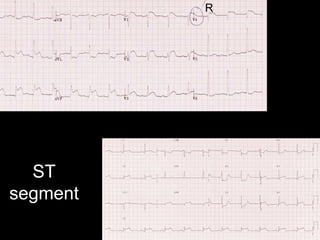
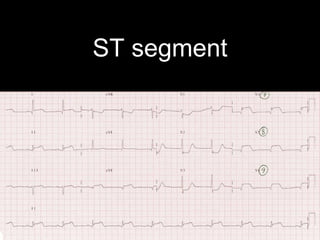
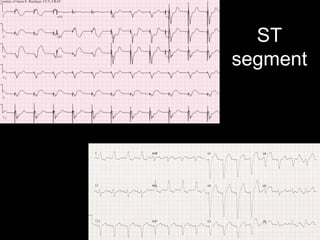
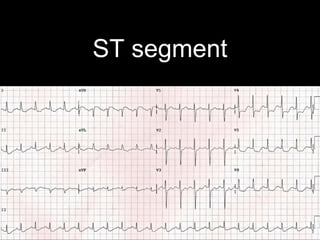
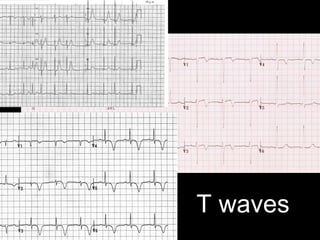
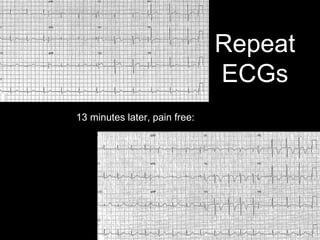
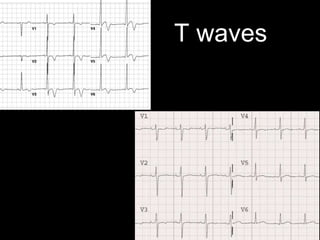
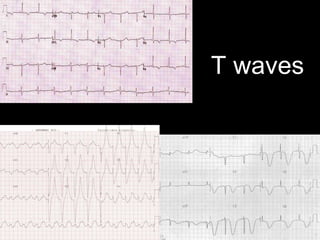
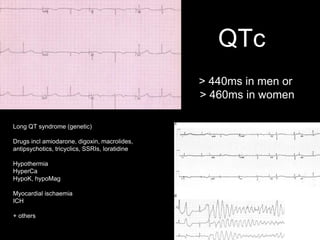
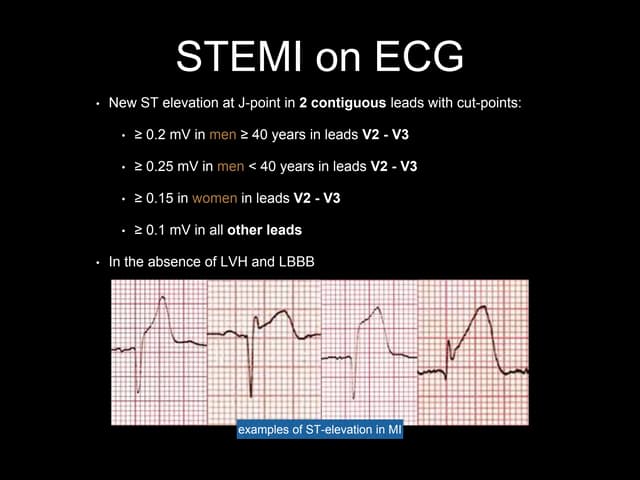
The ECG provides a window into the heart, lungs, electrolytes, body temperature and sometimes the brain. It is important to systematically interpret the ECG by examining features like the rate, rhythm, axes, QRS complex, ST segment, T waves and QTc interval. Interpreting ECGs helps identify conditions like myocardial ischemia, electrolyte imbalances and long QT syndrome. It is important to record the time and name on the ECG and order repeat ECGs as needed to monitor patients.






















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


