This document discusses principles of combat casualty care, including:
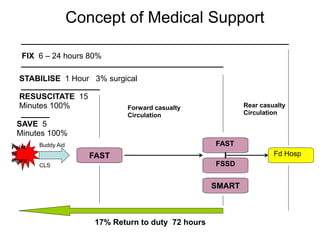
1. The goals of Tactical Combat Casualty Care (TCCC) are to save preventable deaths, prevent additional casualties, and complete the mission.
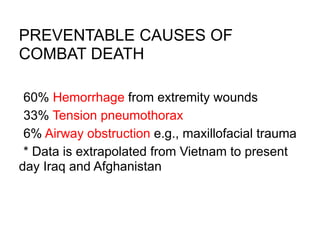
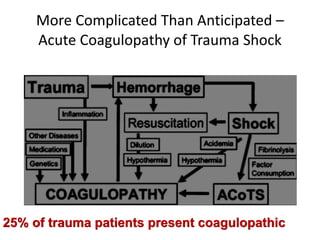
2. About 60% of combat deaths are from hemorrhage from extremity wounds, 33% from tension pneumothorax, and 6% from airway obstruction - all of which can potentially be prevented with the right interventions.
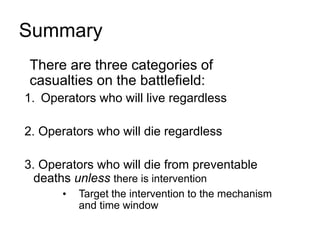
3. There are three categories of casualties on the battlefield - those who will live regardless, those who will die regardless, and those who could be saved from preventable deaths with proper medical intervention. The goal is to target interventions to the correct mechanisms