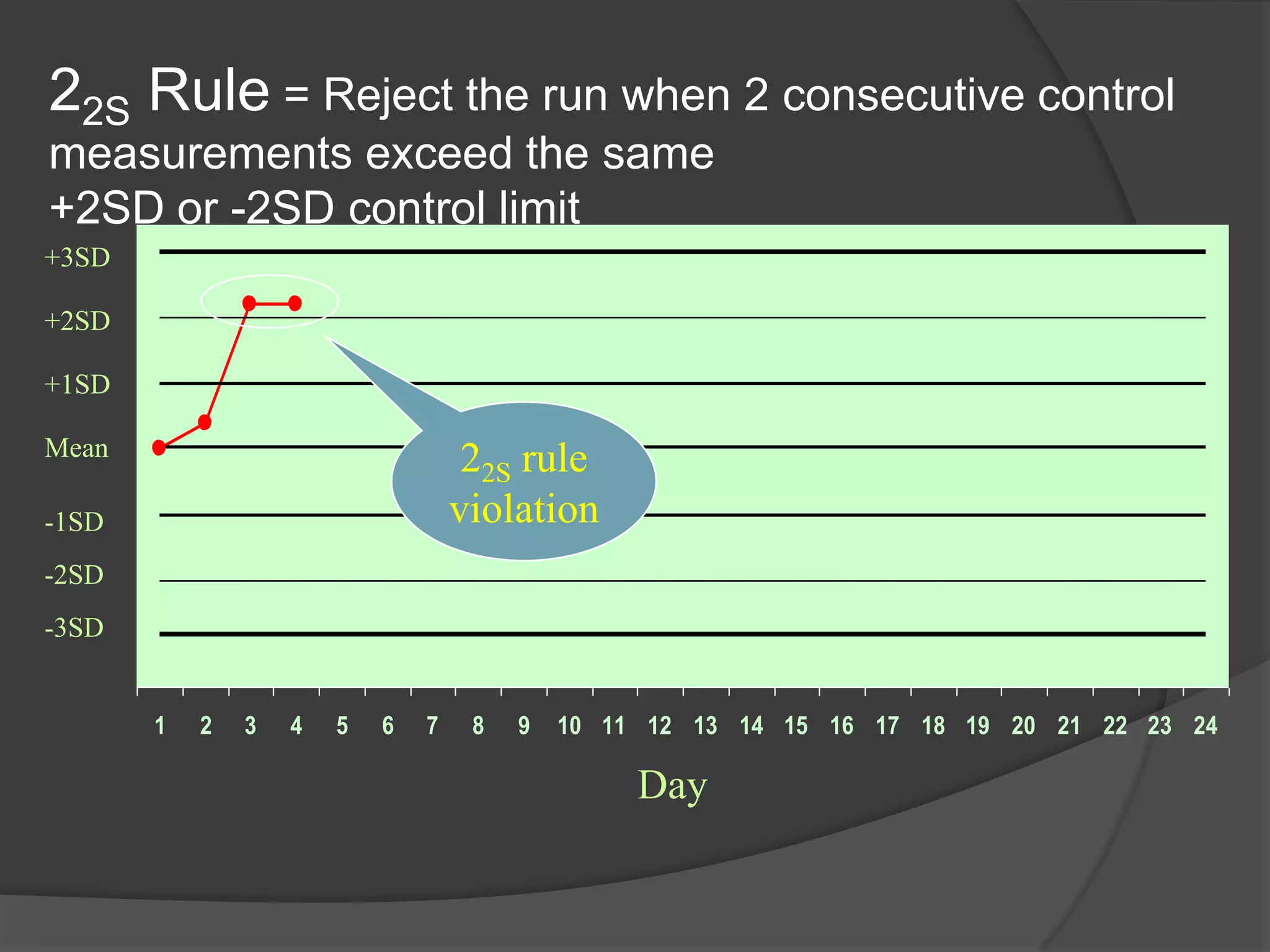
The document discusses quality control, quality assurance, and quality assessment in medical laboratories. It defines each term and describes their related but distinct roles. Quality control refers to statistical processes used during each test run to verify test accuracy and precision. Quality assurance describes the overall program that ensures correct final test results. Quality assessment challenges the quality programs through proficiency testing to evaluate the quality of reported results. The document provides details on quality control measurements and rules to monitor test performance over time and determine if tests are in or out of control.