As teeth age, several changes occur in the major tissues:
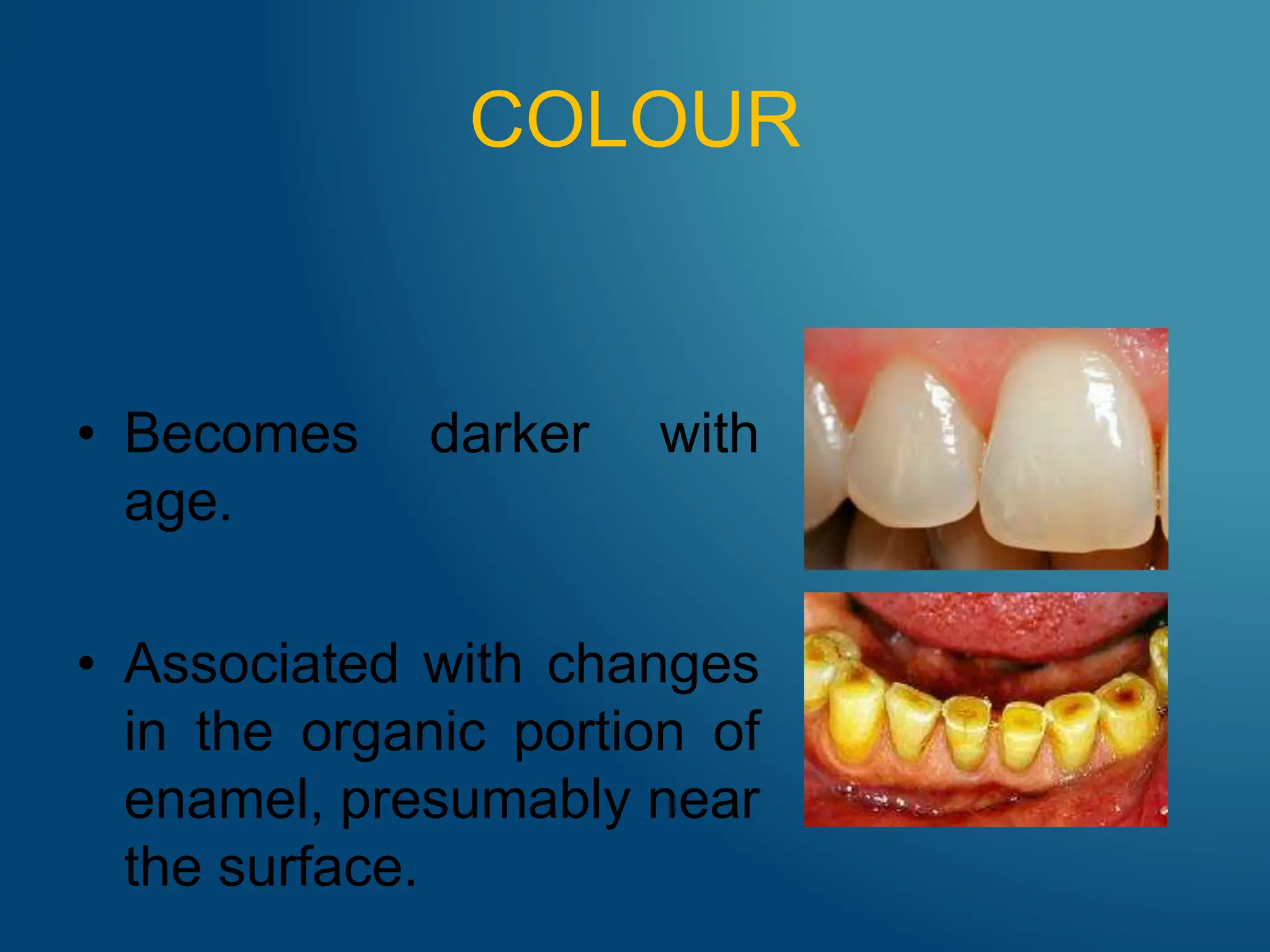
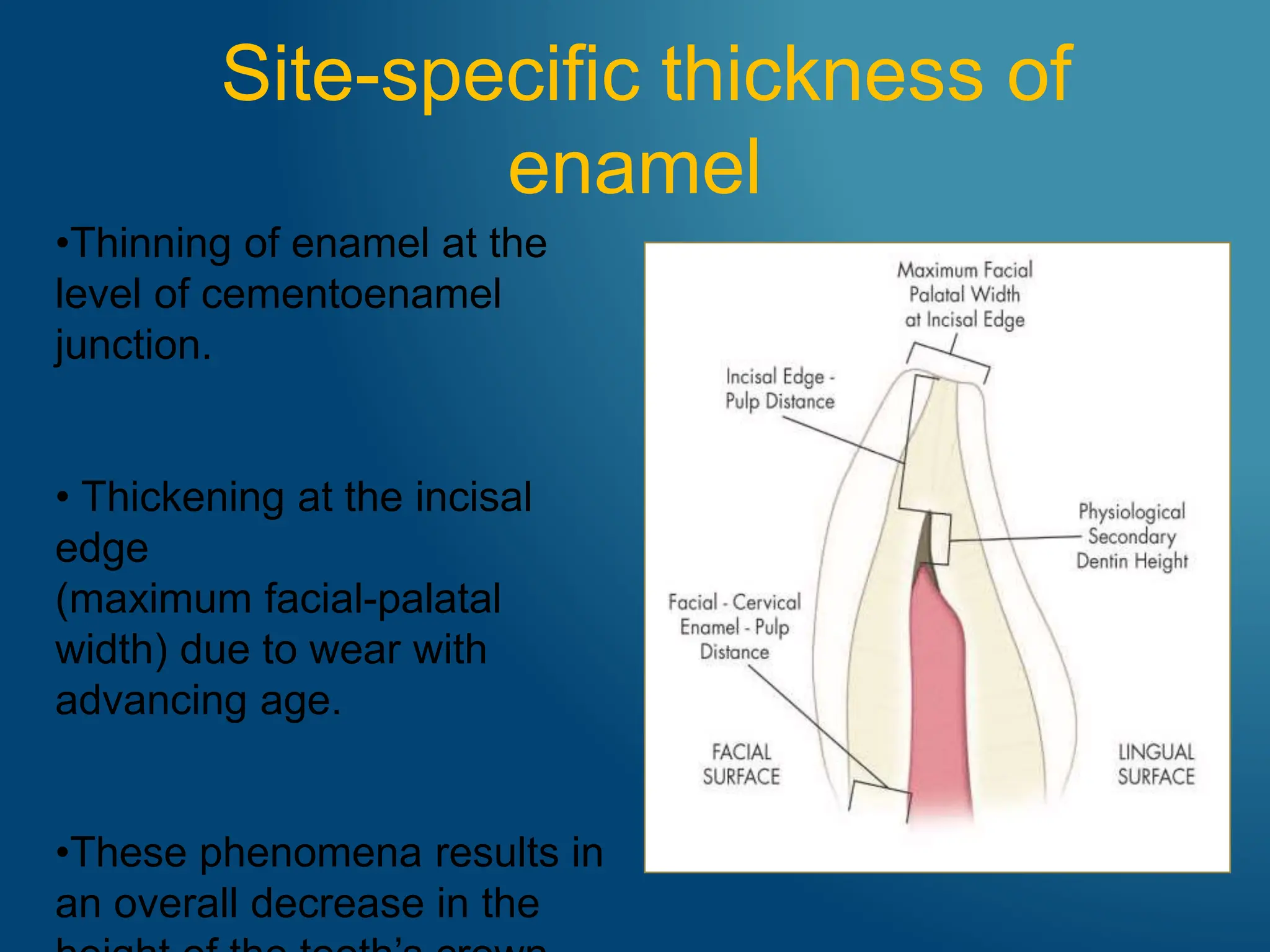
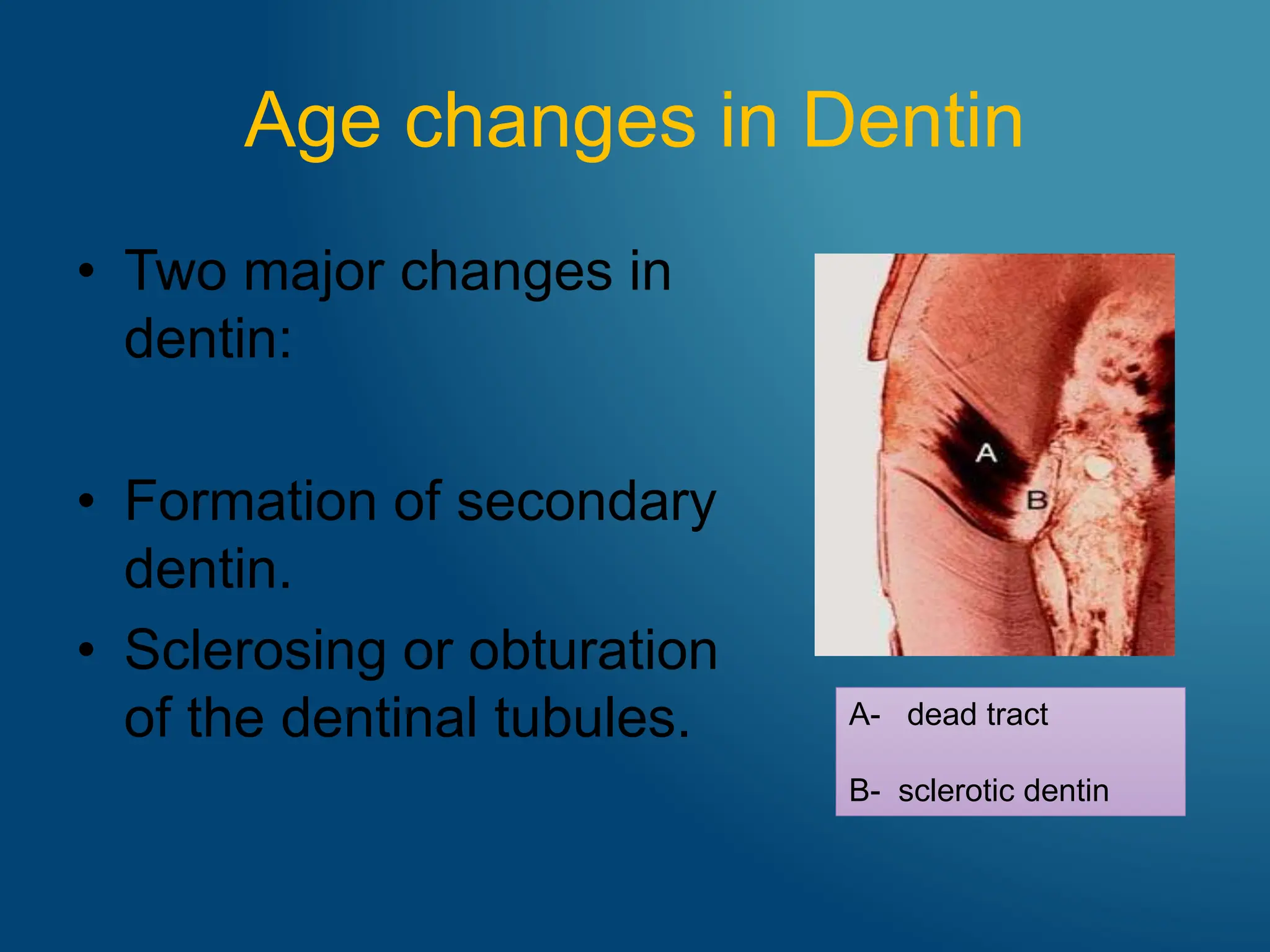
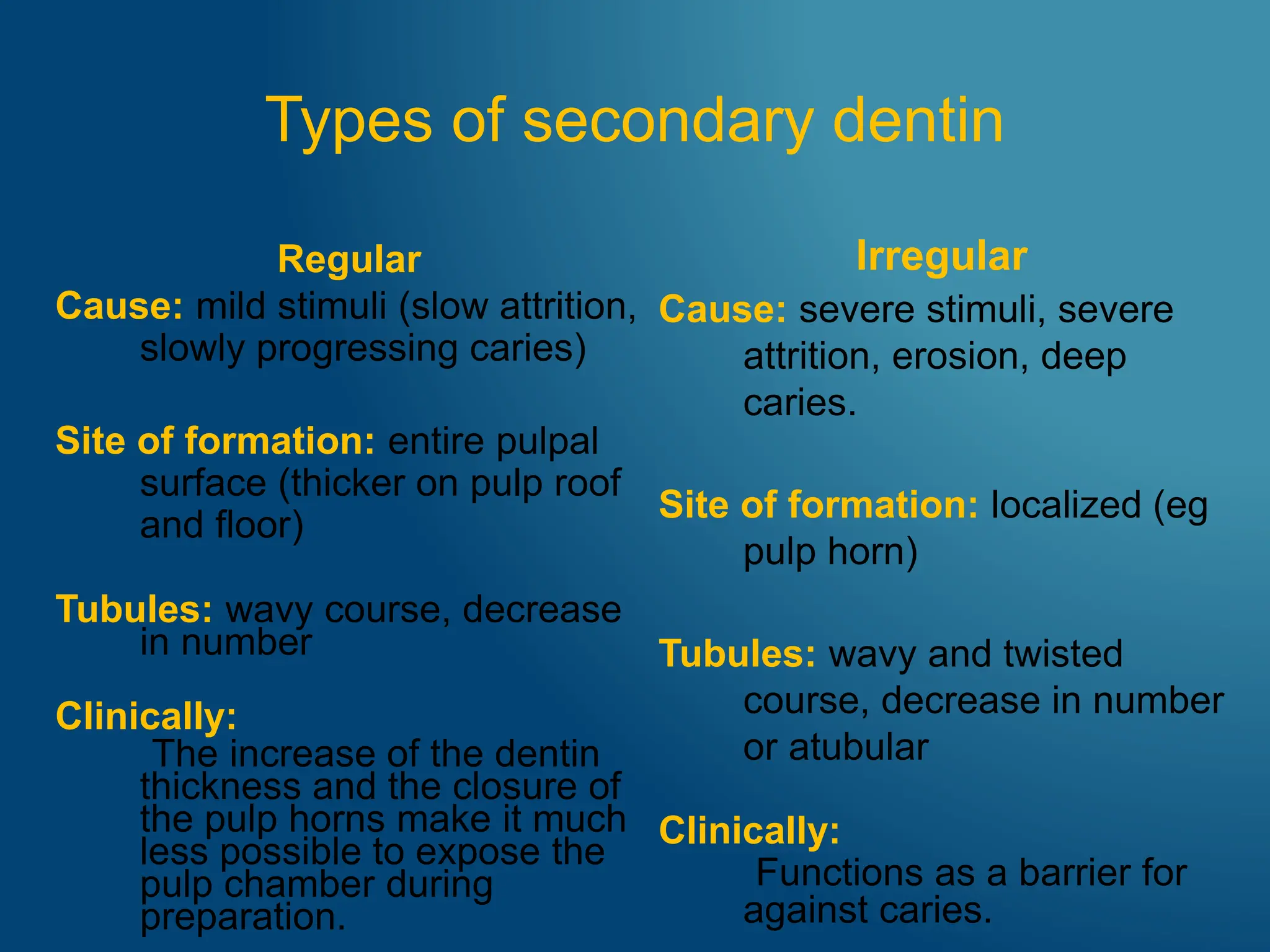
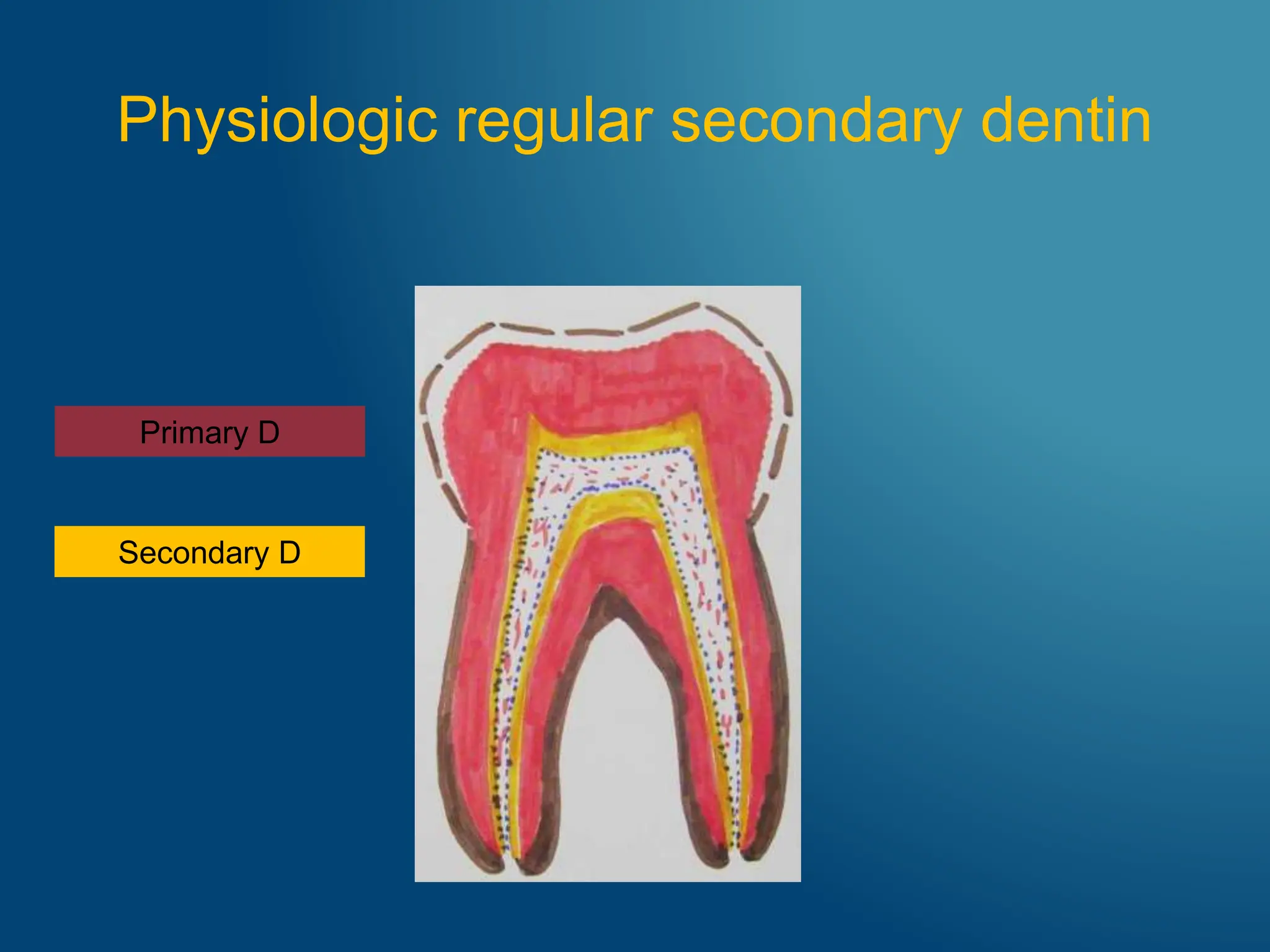
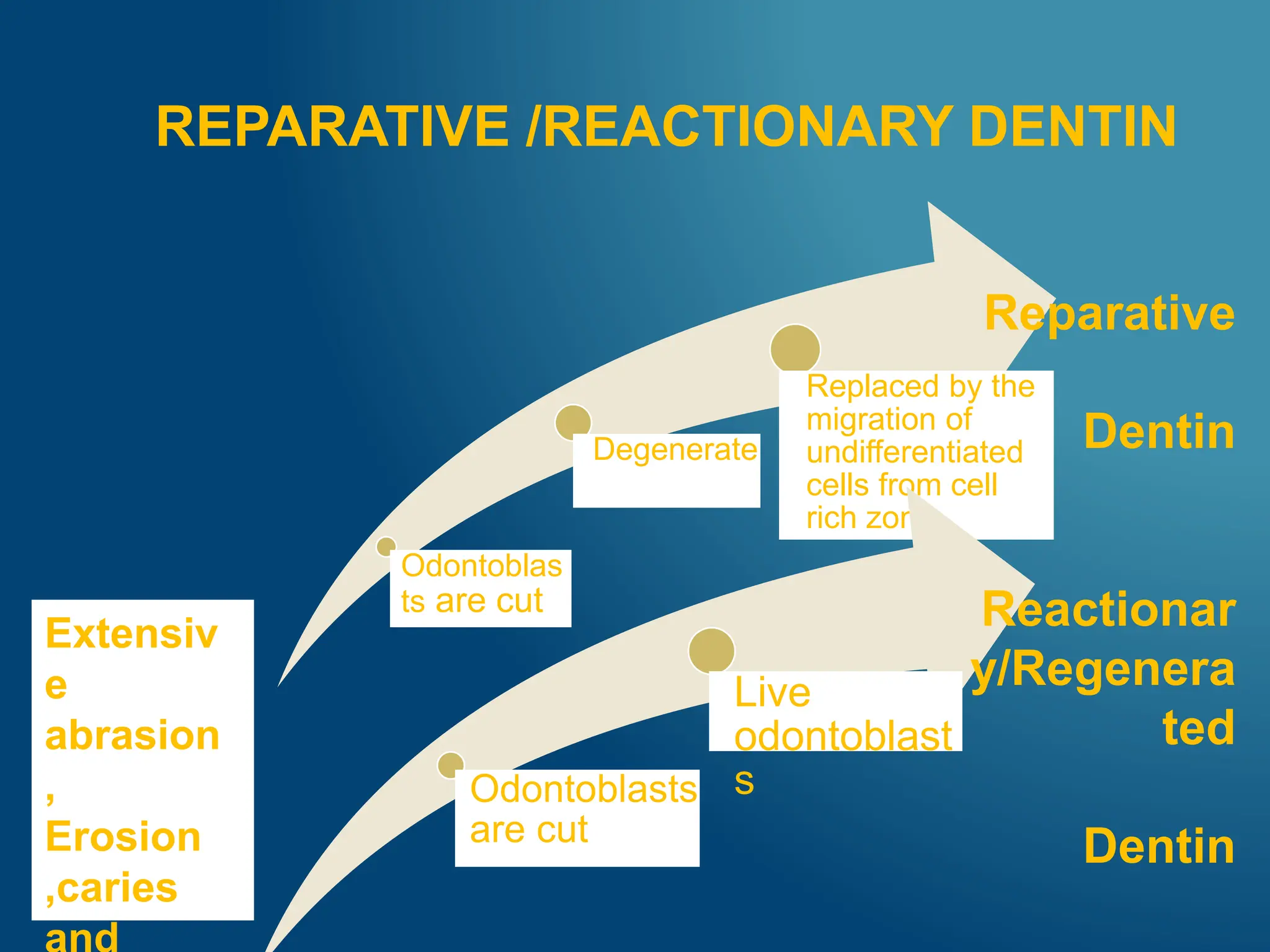
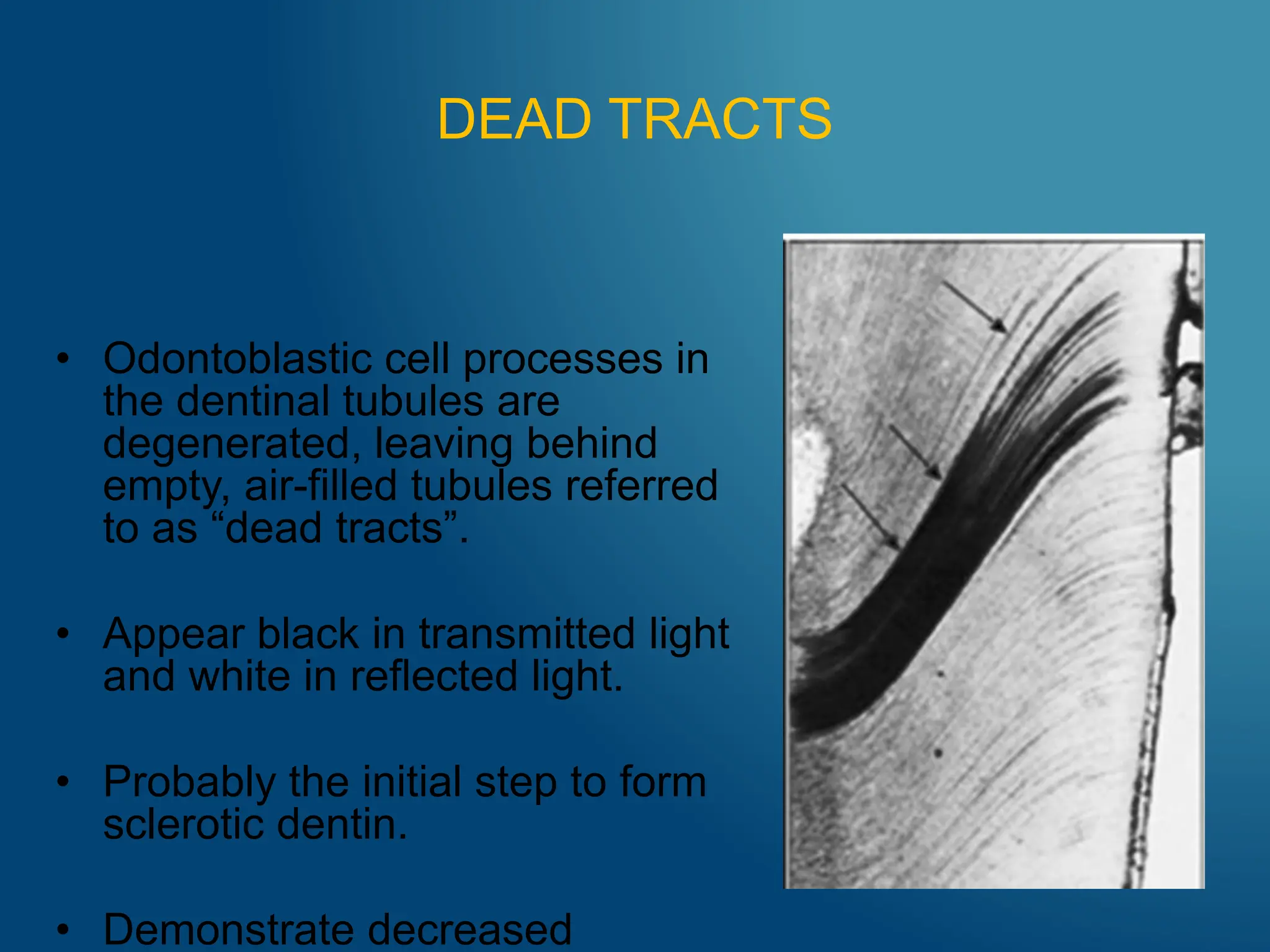
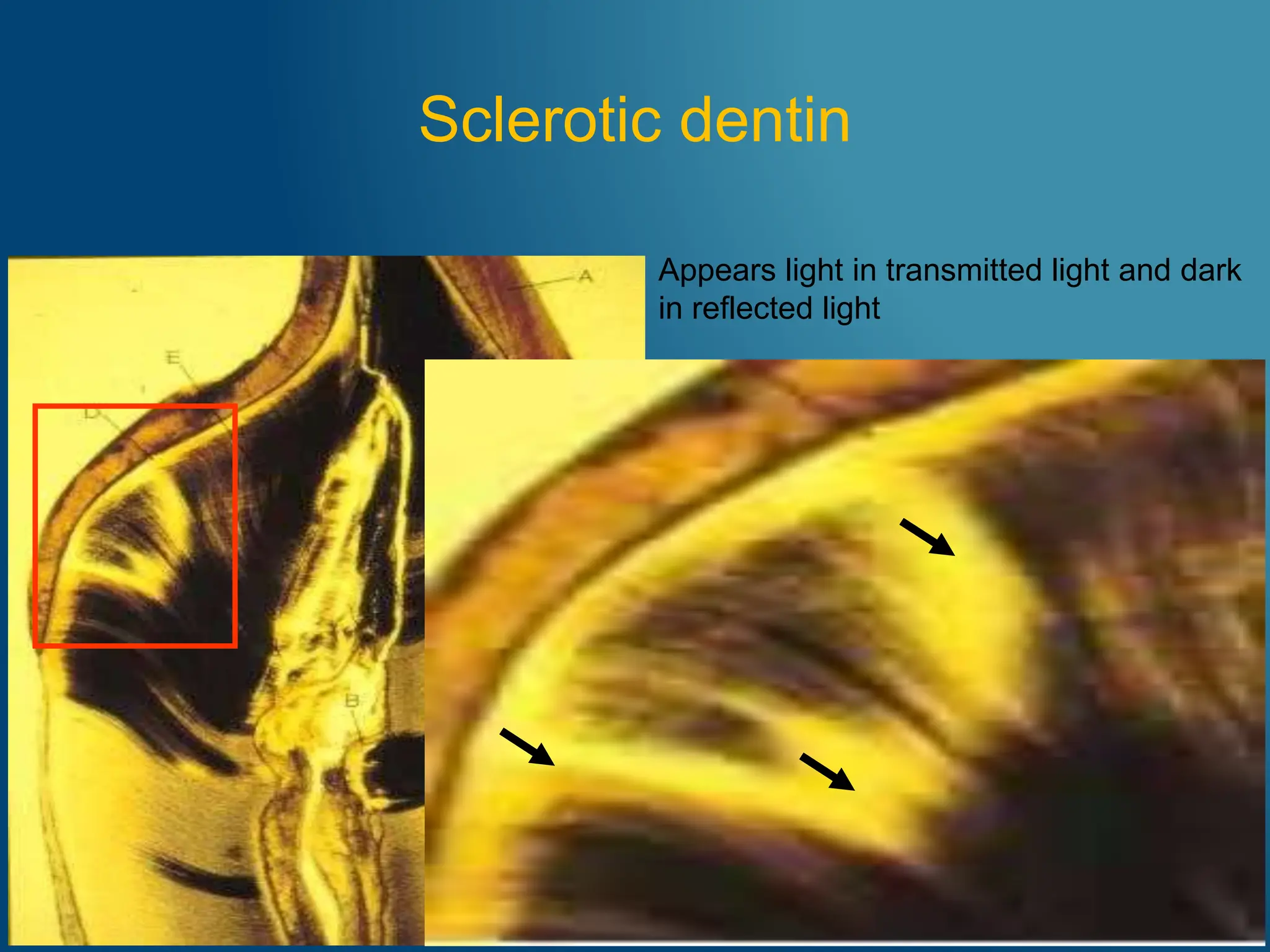
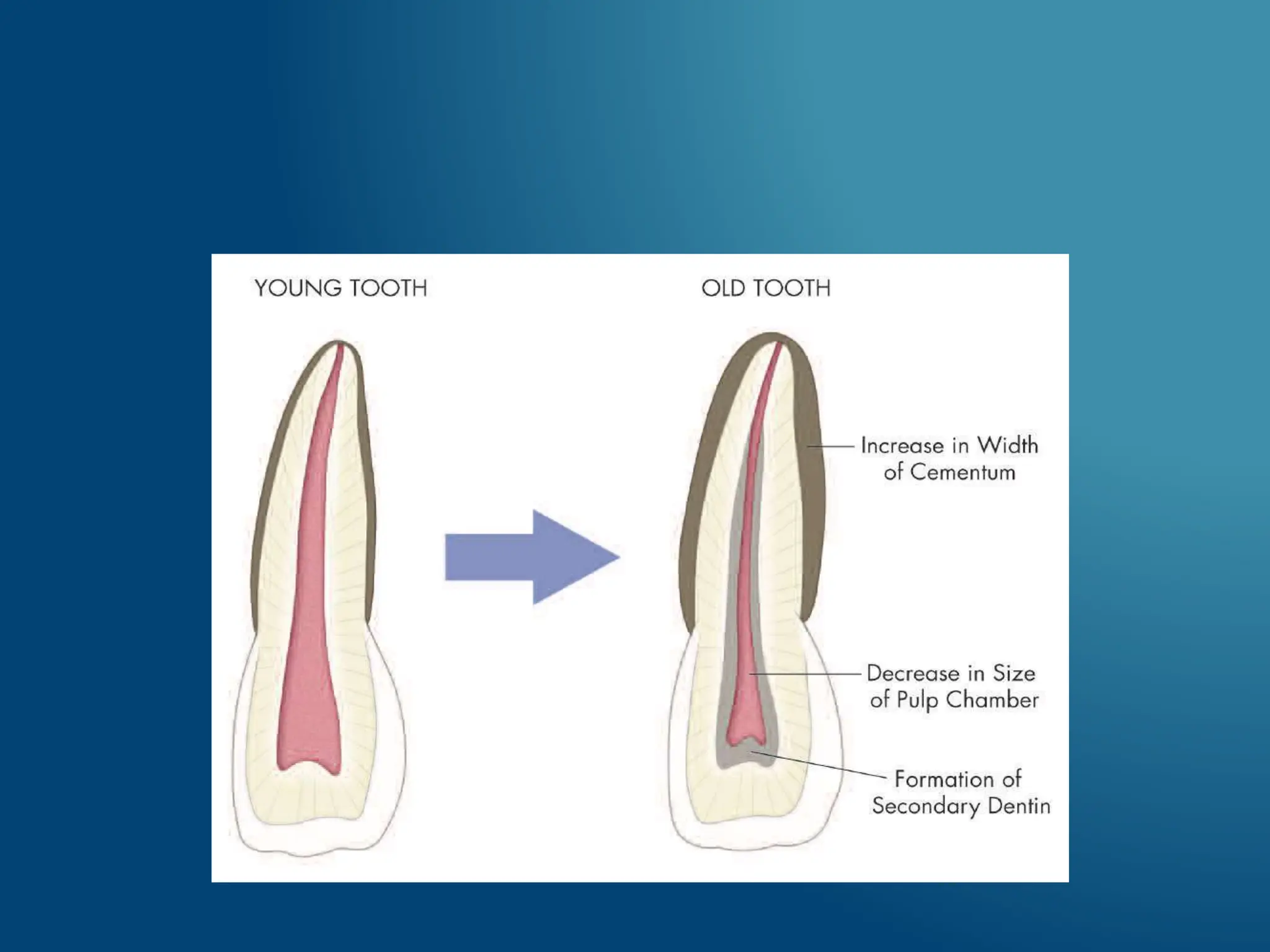
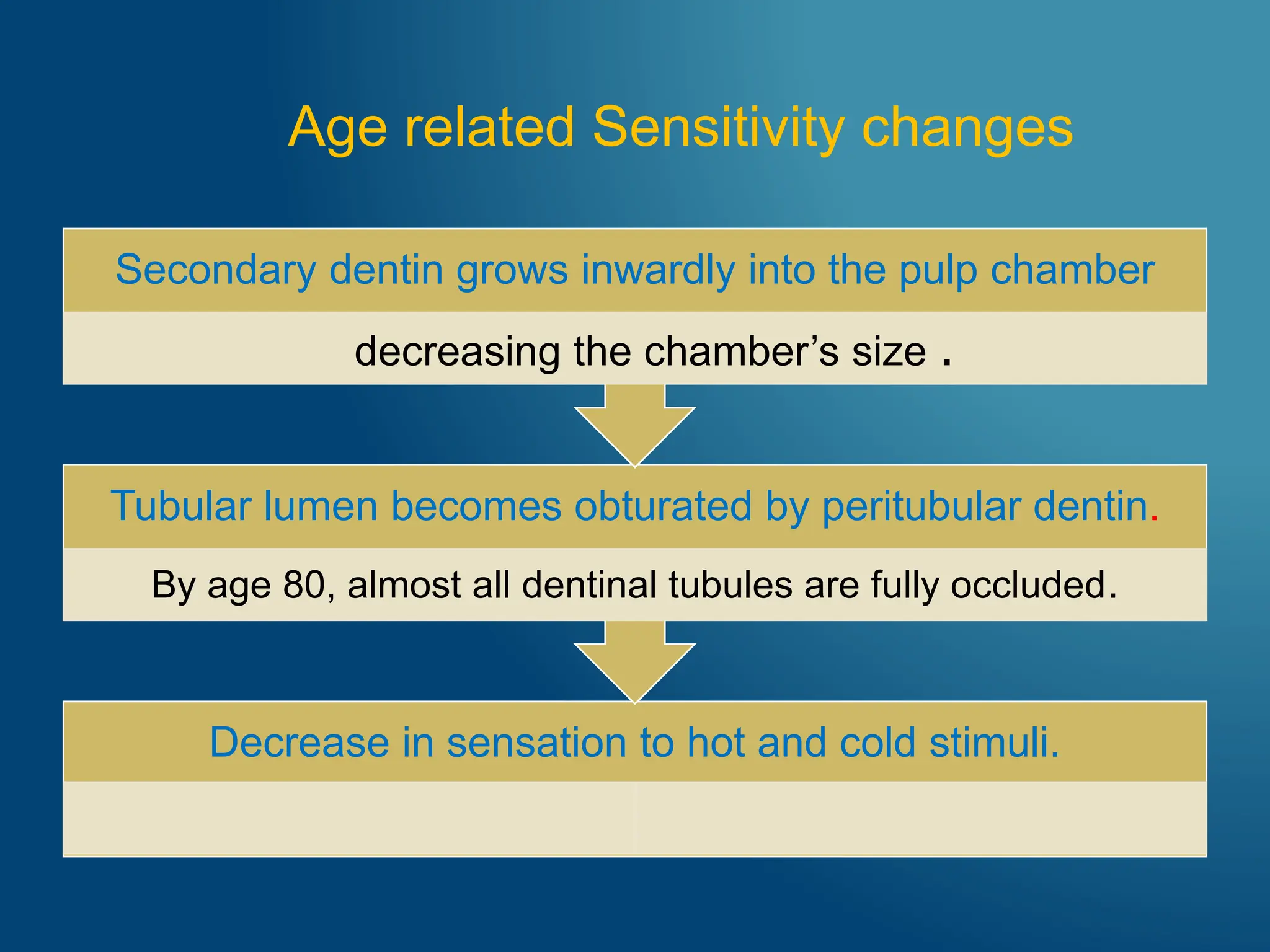
- Enamel becomes darker, develops cracks, and increases in mineral content, making it more resistant to decay. Dentin also increases in mineral content, forming secondary dentin and occluding dentinal tubules. This decreases pulp size and sensitivity. The pulp exhibits decreased cellularity, vascularity, and reparative ability with age. These anatomical and physiological changes are natural aging processes that can impact dental treatment for older patients.












































![Age changes in enamel, dentin and pulp1 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/agechangesinenameldentinandpulp1autosaved-240807163606-82ece9c9-thumbnail.jpg?width=640&height=640&fit=bounds)


















































